In December 2025, an NYU Langone Health surgical team performed what may be the first reported totally endoscopic robotic resection of a retrocardiac paraganglioma.
Led by Didier F. Loulmet, MD, chief of robotic cardiac surgery, Eugene A. Grossi, MD, director of cardiac surgical research, and Costas Bizekis, MD, thoracic surgeon, the team utilized the da Vinci Xi robotic system at every stage, successfully removing the tumor from a woman in her 50s with hypertension and prediabetes.
“It couldn’t happen without an experienced group of surgeons who’ve mastered the complexities of the cardiothoracic anatomy.”
Didier F. Loulmet, MD
The traditional surgical approach to a retrocardiac paraganglioma can be highly invasive, often requiring a cardiac autotransplantation performed through a median sternotomy. Past attempts by surgeons to remove these tumors while keeping the heart in place have largely been unsuccessful—primarily because of the difficult exposure and anatomic complexity of the region behind the heart.
By utilizing a thoracoscopic robotic technique instead, the team eliminated the need for a highly invasive procedure.
“To our knowledge, this represents one of the first reported cases of a completely endoscopic robotic approach for this procedure,” Dr. Loulmet says. “It couldn’t happen without an experienced group of surgeons who’ve mastered the complexities of the cardiothoracic anatomy.”
Surgical Approach
The patient presented with heart palpitations. Initial imaging revealed a large mediastinal mass above the left atrium extending into the subcarinal region with features suggestive of a paraganglioma—a rare neuroendocrine tumor that arises from extraadrenal chromaffin cells.
“It is rare for these tumors to occur behind the heart,” notes Dr. Loulmet. “Although not malignant, its continued growth would have led to complications due to compression of vital structures and the secretion of catecholamines.”
Upon further imaging, Dr. Bizekis confirmed attachment of the tumor to the left atrium, warranting the involvement of cardiac surgery. Coronary CT angiography also revealed external compression of the left atrium and upper pulmonary vein—further complicating the case.
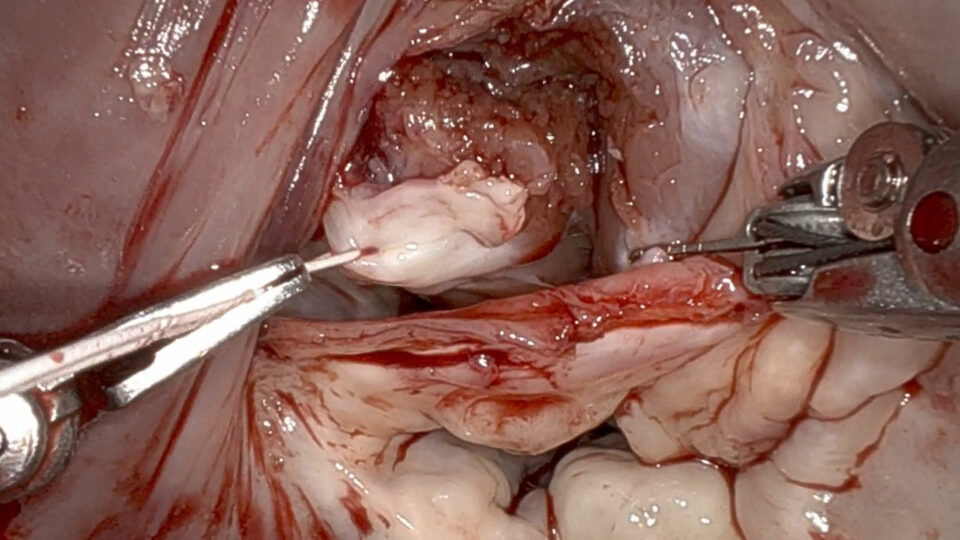
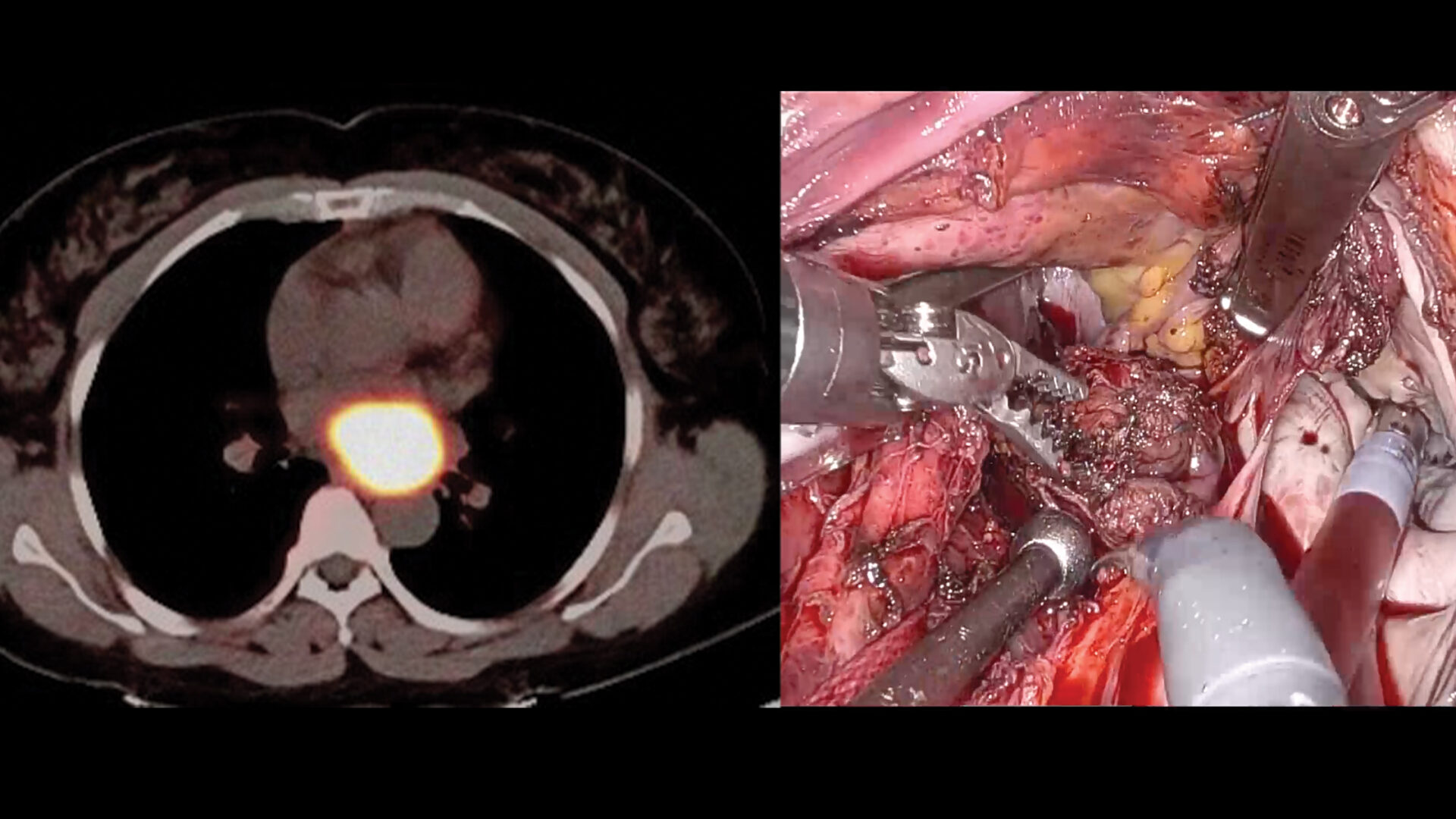
The operation involved placement of five side ports through the right chest wall. Following dissection between the back of the heart and the spine, a 5-cm tumor was identified attached to the roof of the left atrium and extracted.
Due to thinning or tearing of the left atrial roof, the atrial wall was replaced with a bovine pericardial patch sewn between the right and left pulmonary veins. A sample of the mass was sent to pathology for review.
“Our experience gave us the confidence to approach this case robotically, minimizing complications and hastening recovery for the patient.”
Costas Bizekis, MD
“After careful planning, our experience gave us the confidence to approach this case robotically, minimizing complications and hastening recovery for the patient,” Dr. Bizekis says.
After surgery, the patient was transferred to the ICU in stable condition and recovered without complications. She was discharged to Rusk Rehabilitation seven days later before returning home.
Mastering the Technique
According to Dr. Loulmet, a key to the success of the procedure was his years of seamless collaboration with Dr. Grossi across hundreds of robotic cardiac surgery cases. “Our experience and ability to communicate while using the robot was vital to the success of this case,” explains Dr. Loulmet.
The team is now refining the technique for patients with similar presentations, aiming to establish its long-term feasibility and safety.
“We’re excited to continue to push the envelope in robotic approaches for similar situations,” says Dr. Loulmet.
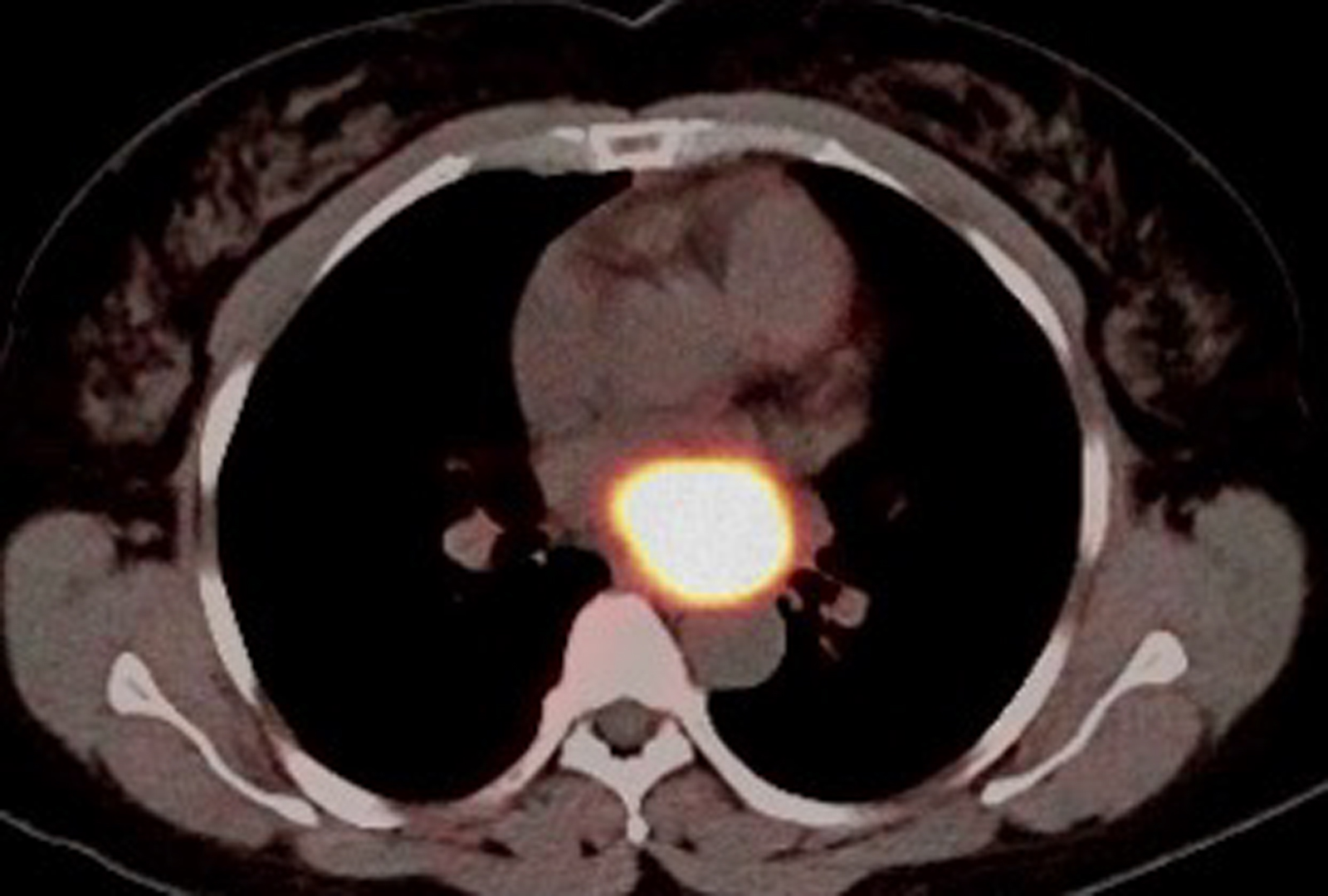
PET scan showing intense somatostatin receptor (SSTR) expression consistent with paraganglioma. Source: NYU Langone Health
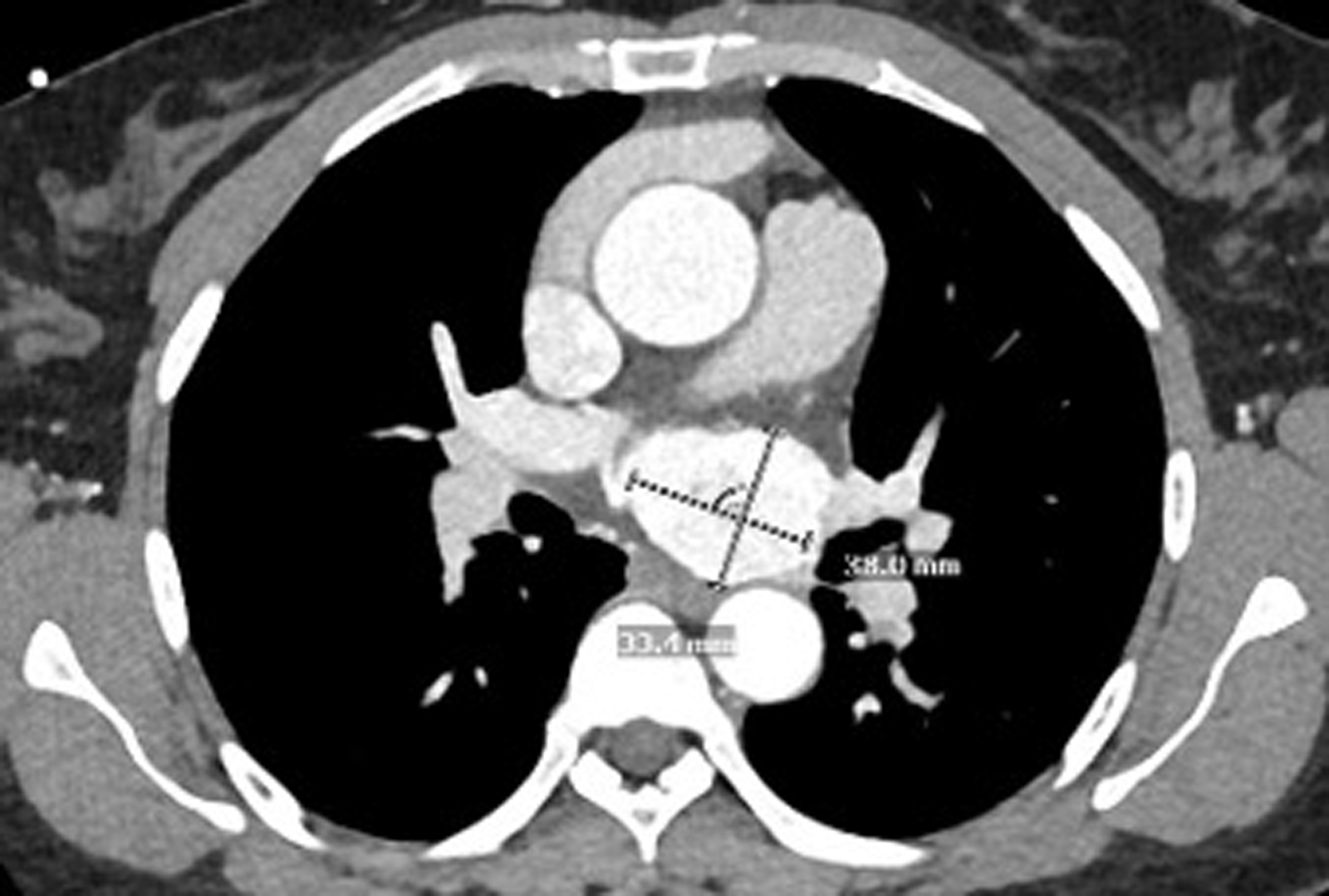
Preoperative CTA showing the tumor location relative to the spine, aorta, and pulmonary veins. Source: NYU Langone Health
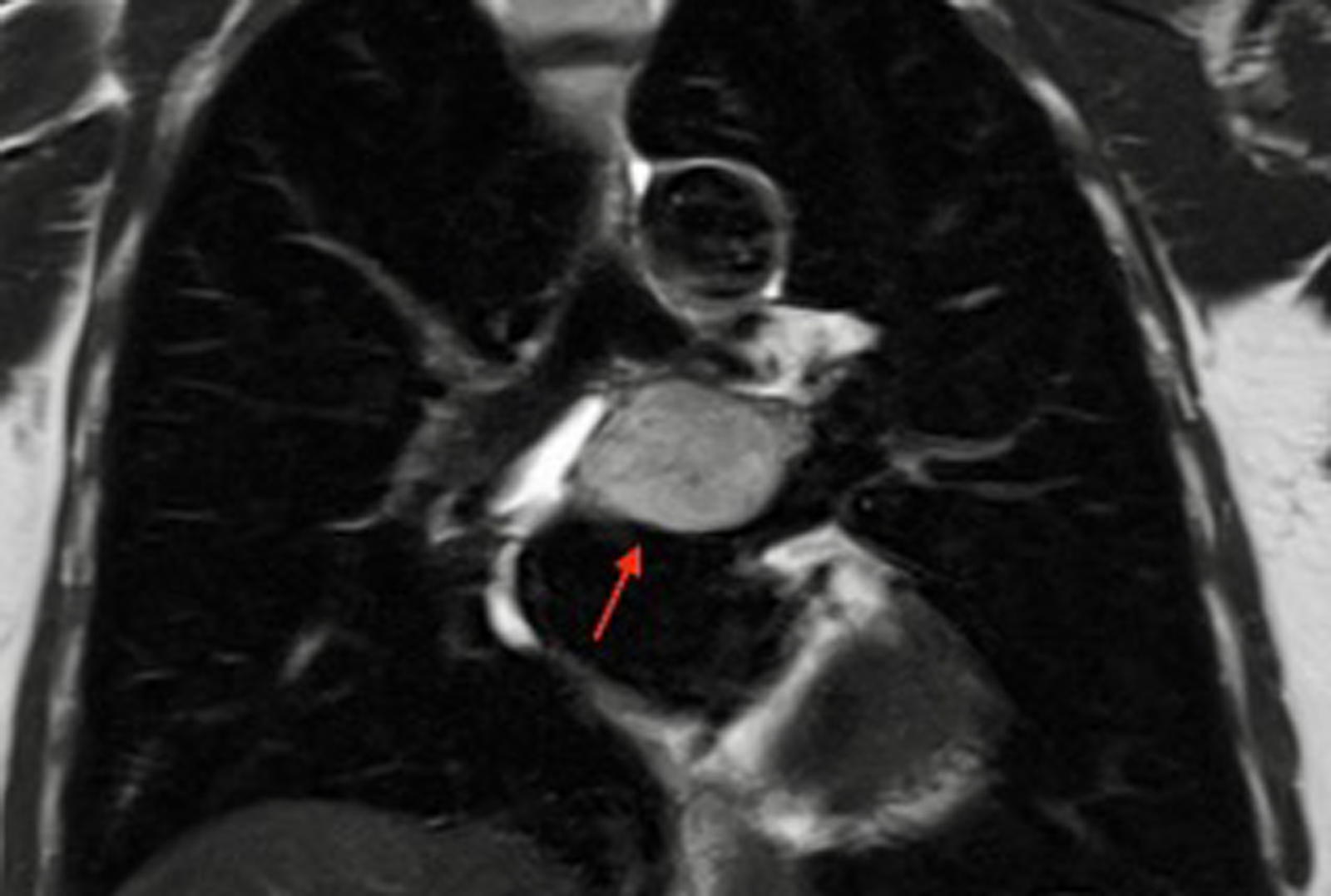
Preoperative MRI revealing the tumor below the tracheal bifurcation. Source: NYU Langone Health