Management of intermediate favorable risk prostate cancer (IFRPCa) often requires balancing the risk of under-treatment associated with active surveillance (AS) against the potential morbidity of definitive whole-gland treatment. For carefully selected men with MRI-visible, unilateral Grade Group 2 (GG2) disease, focal therapy (FT) may provide a middle ground between these competing approaches.
This case highlights the long-term oncologic and functional outcomes of a patient with MRI-concordant GG2 prostate cancer who underwent focal cryoablation (FCA) in 2019 after declining radical prostatectomy (RP) and radiation therapy (RT). More than seven years after treatment, he remains free of clinically significant recurrence with preserved urinary continence and sexual function, illustrating the potential role of FCA in appropriately selected patients.
Case Highlights:
- A man in his mid-50s with rising PSA and MRI-concordant GG2 prostate cancer elected FCA to avoid the potential morbidity of RP or RT.
- PSA declined from 18 ng/mL pretreatment to 0.2 ng/mL at six months and has remained stable at 0.3 ng/mL through nearly seven years of follow-up.
- Despite a suspicious MRI finding at two years, serial MRI examinations and targeted/systematic biopsies have demonstrated no evidence of clinically significant recurrence.
Case Presentation
A patient in their mid-50s presented to NYU Langone in March 2019 with a rising PSA and low volume GG2 disease. The PSA levels were as follows:
| Date | PSA Level (ng/mL) |
|---|---|
| 01/2017 | 11.5 |
| 06/2017 | 13 |
| 11/2017 | 13.5 |
| 03/2019 | 18 |
In 2017, a 12-core systematic biopsy (SB) showed GG2 disease only in a right apical core biopsy. An MRI was not performed prior to the SB. He was counseled to undergo RP or RT. He elected AS in order to avoid treatment-related complications of whole gland treatments.
In April 2019, at NYU Langone, an MRI demonstrated a 21 x 12 mm PI-RADS 3 lesion in the right anterior mid-gland transition zone and a 14 x 9 mm PI-RADS 2 lesion in the right posterolateral mid-gland peripheral zone (Figure 1). There was no evidence of extraprostatic extension, seminal vesicle invasion, or pelvic adenopathy. The prostate volume was 28 cc.
The patient had no family history of prostate cancer, an International Prostate Symptom Score (IPSS) of 7, and a Sexual Health Inventory for Men (SHIM) score of 25.
Our standard biopsy protocol was subsequently performed, which included four targeted biopsies of all MRI regions of interest and a SB. The findings were as follows:
- Targeted biopsy of the PI-RADS 3 lesion in the right anterior mid-gland transition zone revealed prostate adenocarcinoma with a Gleason score of 3+4=7 (GG2), including 10 percent pattern 4 disease. Cancer involved approximately 15 percent of the sampled tissue, measuring 2 mm in greatest dimension.
- Targeted biopsy of the PI-RADS 2 lesion in the right posterolateral mid-gland peripheral zone demonstrated prostate adenocarcinoma with a Gleason score of 3+3=6 (GG1), involving 10 percent of the sampled tissue (1 mm).
- A standard 12-core SB was performed under ultrasound guidance according to the Artemis-derived template identified a single positive core from the right medial mid prostate containing Gleason score of 3+3=6 (GG1) disease involving 10 percent of the tissue sampled (1 mm).
The patient was counseled that standard treatment for GG2 disease at the time was RP or RT. However, he remained averse to whole gland treatment if a reasonable alternative would decrease risks of treatment-related complications. Because clinically significant disease appeared confined to the right prostate on MRI and targeted/systematic biopsy, he was considered an appropriate candidate for FT. The ipsilateral low-risk disease was felt to be clinically insignificant and expected to be eradicated with ablation of the right anterior transition zone (TZ) disease.
After discussion of our two-year experience with FCA, he elected to proceed with treatment. Because the MRI target and csPCa were located in the anterior TZ, HIFU was not offered.
Focal Cryoablation
In May 2019, FCA was performed under general anesthesia with four cryoprobes: one right anterior, two right posterior, and one left anterior. The treatment plan was designed to ablate the entire right lobe. An additional probe was placed in the left TZ to ensure margin control. The probes were positioned to limit thermal injury to the right neurovascular bundle. Two freeze cycles were performed, and the patient was discharged the same day.
Follow-Up
Six-Month Follow-Up. At six months, that patient’s PSA had declined to 0.2 ng/mL, with an IPSS of 3 and a SHIM score of 25. His erections returned to baseline and lower urinary tract symptoms (LUTS) improved. He experienced no urinary incontinence, although semen volume was markedly decreased. MRI showed no evidence of disease recurrence.
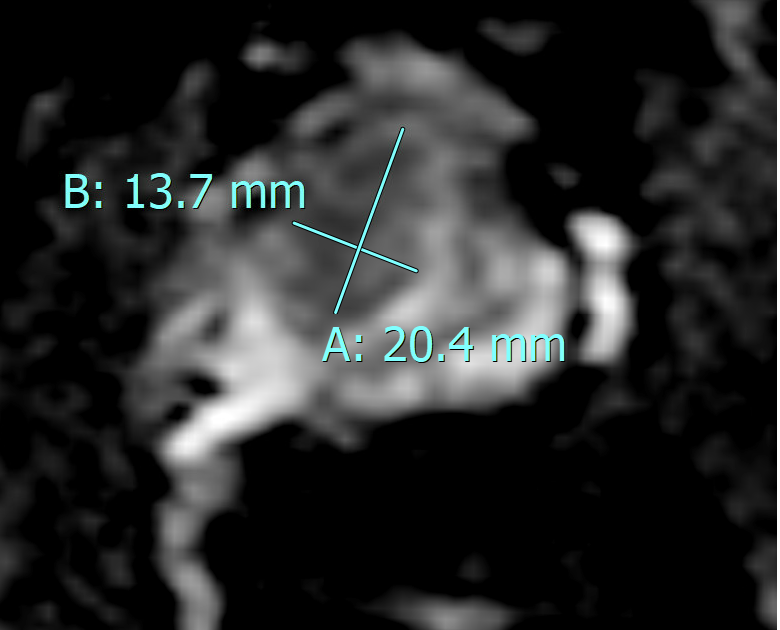
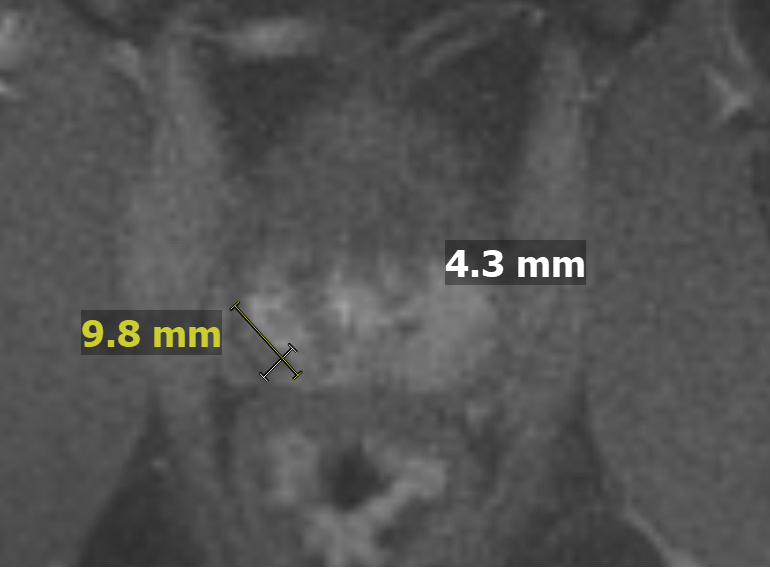
Twenty-Four-Month Follow-Up. At 24 months, the PSA was 0.3 ng/mL and MRI demonstrated a 1-cm stable ablation cavity and a 0.8 x 0.6 cm enhancing focus in the right posteromedial peripheral zone at the superomedial aspect of the ablation cavity in the mid gland, suspicious for local recurrence (Figure 2).
Despite an extremely low PSA level, a prostate biopsy was performed with six cores targeting the MRI “suspicious target” and a 14-core SB. All biopsies were benign showing only treatment effect.
Long-Term Surveillance. The patient was compliant with our surveillance protocol, which involved PSA testing every six months and MRI at six months and years 2, 3.5, and 5.
The five-year MRI showed no suggestion of disease recurrence. On the most recent follow up visit in February 2026, the patient’s PSA was 0.3 ng/mL, with an IPSS of 11 and SHIM score of 25. He reported no erectile dysfunction and was not taking a PDE5 inhibitor.
The 7.5-year MRI is scheduled for August 2026.
Discussion
The goal of treating clinically localized prostate cancer is to prevent development of metastatic disease and prostate cancer mortality. Contemporary AUA/ASTRO/SUO1 and EAU/ESTRO/SIOG2 guidelines recommend a wide range of treatment options for intermediate favorable risk disease including AS, RP, and RT. Despite extensive literature validating FT for focal prostate cancer, current guidelines consider FT investigational and recommend that it be offered within a clinical trial. Beginning in 2017, we have enrolled over 600 men in a clinical trial investigating FCA for patients with focal disease identified by MRI and prostate biopsy. The patient presented in this case is enrolled in this clinical trial.
The decision to offer AS, RP, RT, or FT must balance the potential consequences of delayed treatment associated with AS against the unnecessary morbidity of immediate RP and RT.
Five-Year Outcomes with FCA. MRI coupled with MR fusion targeted and SB has enabled the detection of “focal” IFRPCa (GG2).3 We have previously reported 70 percent five-year csPCa recurrence-free survival for men with intermediate risk disease (both GG2 and GG3) following FCA.4 Only 11 percent of these men underwent whole gland salvage treatment (WGST) at five years.
A unique strength of this study was 91 percent compliance with our rigorous oncological surveillance protocol at five years. These encouraging oncological outcomes were achieved without incontinence or rectal injury, with improvement in LUTS for men presenting with moderate to severe symptoms, minimal treatment regret, and rates of sexual dysfunction markedly less than RP and RT.5,6,7
Seven-Year Outcomes with FCA. Between May 2017 and June 2025, 276 subjects with MRI concordant IFRPCa (GG2) were enrolled in the study, which was presented at AUA 2026 and has been accepted for publication in Urology. Overall, 39 men (14.1 percent) developed csPCa recurrence. Of these recurrences, 11 were in-field only, 18 out-of-field only, and 10 involved both in-field and out-of-field recurrence. In total, 21 men experienced in-field recurrence and 28 experienced out-of-field recurrence.
The total csPCa recurrence-free survival at three, five, and seven years were 90.20 percent, 78.36 percent, and 70.31 percent, respectively. In-field csPCa recurrence-free survival at three, five, and seven years was 94.55 percent, 87.04 percent, and 80.94 percent, respectively. Out-of-field csPCa recurrence free survival at three, five, and seven years was 92.90 percent, 84.62 percent, and 77.78 percent, respectively.
The time-dependent increase in rates of csPCa recurrence mandates long-term oncological surveillance. The rate of biochemical recurrence for IFRPCa following RP at 10 years is approximately 20 percent.8 We therefore interpret our rates of csPCa recurrence-free survival up to seven years to validate FCA for men with IFRPCa based on oncological outcomes.
Freedom from failure (FFF) was defined as freedom from prostate cancer mortality, development of metastasis, or WGST. There were no prostate cancer mortalities, three patients developed metastases, and 21 underwent WGST. Overall, FFF was observed in 92.03 percent of men with IFRPCa. FFF rates at three, five, and seven years was 95.35 percent, 85.74 percent, and 84.31 percent, respectively.
None of the subjects experienced any level of urinary incontinence, rectal injury, or received neoadjuvant ADT. No patient required hospital admission postoperatively or within 30 days of treatment.
During follow-up, seven men died of causes unrelated to prostate cancer and were censored at the time of death.
When we initiated the clinical trial in 2017, MRI and prostate biopsy were mandated at six and 24 months. We have subsequently reported that protocol biopsy can be safely avoided at all time points if MRI is not suspicious for disease recurrence and PSA is not progressively increasing.9,10
Conclusion
Several studies evaluating AS in men with GG2 disease show conflicting outcomes. In the PROTECT trial, the 15-year rates of prostate cancer mortality among men with GG2 disease randomized to AS, RP, and RT were 4.3 percent, 4.9 percent, and 5.0 percent, respectively.11 In the Sunnybrook AS cohort, men with IFRPCa exhibited a 3.7-fold greater risk of developing metastasis at 15 years compared with men with GG1 disease.12 Based on these findings, treating the patient presented in this case—a man in his mid-50s with GG2 disease associated with a large MRI target—would be ill advised.
If the concern is that AS represents under-treatment while RP or RT represents over-treatment for IFRPCa, then men like the one discussed in this case may represent optimal candidates for FT.
Our experience with FCA is approaching 10 years and unequivocally supports FCA as a very reasonable option for men with IFRPCa associated with an MRI target with no evidence of extra-capsular extension or distal apical disease on MRI, and no contralateral GG> 1 disease. FCA may be the preferred shared-decision treatment option for these men when both the patient and surgeon/radiation oncologist are concerned that AS may represent under-treatment and RP/RT may represent over-treatment.
References
- Sanda MG, et al. J Urol. 2018;199(4):990-997. DOI.
- Mottet N, et al. Eur Urol. 2017;71(4):618-629. DOI.
- Kenigsberg AP, et al. Urology. 2018;112:121-125. DOI.
- Lepor H, et al. Urology. 2025;196:189-195. DOI.
- Thakker S, et al. Can J Urol. 2022;29(3):11128-11135. Link.
- Wysock J, et al. Urology. 2023;171:158-163. DOI.
- Lepor H, et al. Urol Oncol. 2025;43(6):398.e1-398.e6. DOI.
- Epstein JI, et al. Eur Urol. 2016;69(3):428-435. DOI.
- Lepor H, et al. BJU Int. 2025;136(3):447-451. DOI.
- Lepor H, et al. J Urol. [Internet]. 2025 May 1;213(5S):e1166. DOI.
- Hamdy FC, et al. N Engl J Med. 2023;388(17):1547-1558. DOI.
- Klotz L, et al. J Clin Oncol. 2015;33(3):272-277. DOI.