End-stage ankle arthritis is a debilitating condition affecting nearly 1 percent of the adult population.1,2 Approximately 80 percent of ankle arthritis cases are post-traumatic and frequently are associated with progressive deformity and joint instability.1,3,4
Cavovarus deformity represents a particularly challenging subset of ankle arthritis because varus malalignment shifts load medially across the tibiotalar joint, accelerating asymmetric cartilage degeneration and contributing to progressive instability and pain. Historically, severe coronal plane deformities, particularly varus deformities greater than 10 to 15°, were considered a relative contraindication to total ankle replacement (TAR) due to concerns regarding implant malalignment, instability, and early component failure.5,6 As a result, many of these patients were treated with ankle arthrodesis.
Advances in implant design, improved instrumentation, and increased experience with deformity correction have expanded the indications for TAR. Contemporary studies have demonstrated that satisfactory clinical and radiographic outcomes can be achieved in ankles with significant coronal plane deformity when appropriate alignment and ligament balance are restored.5,7,8 Today, deformities exceeding 20° may be treated successfully with TAR when ancillary procedures are performed to correct alignment and achieve joint stability.9 Correction often requires a combination of procedures including soft-tissue releases, tendon lengthening, ligament reconstruction or imbrication, and osseous procedures such as calcaneal or midfoot osteotomies to address multiplanar deformity.5,10,11
Here, we present a case of end-stage ankle arthritis associated with severe cavovarus deformity successfully treated with single-stage surgery involving a TAR combined with extensive soft-tissue balancing and corrective osteotomies to achieve multiplanar deformity correction and a stable plantigrade foot.
Case Highlights:
- The patient had a hindfoot–ankle varus deformity of 40° with forefoot abduction and midfoot cavus due to a plantarflexed first ray.
- The single-stage surgery included TAR, tendon procedures, subtalar fusion, multiplanar osteotomies, and ligament balancing.
- At six months postoperatively, the patient was able to walk up to two miles per day and demonstrated ankle range of motion of 10° dorsiflexion and 30° plantarflexion.
- At two-year follow-up, the patient had neutral foot and ankle alignment, pain-free ankle motion, and complete healing of all fusions and osteotomies.
Patient Case
A man in his late 60s presented with progressive discomfort affecting his left foot and ankle. He had a background of polio in childhood which resulted in severe muscle imbalance, peroneal weakness and a partially correctable equino-cavovarus deformity. His main symptoms included debilitating global ankle pain and swelling, chronic ankle instability recalcitrant to bracing and steroid injections, and progressive lateral midfoot pain centered over the fifth metatarsal base. He hoped that one day, he would be able to walk on a beach.
Clinical examination demonstrated an antalgic gait pattern with shortened stance phase and limited ankle rocker motion. There were multiple well-healed incisions from corrective surgery as a child. His hindfoot–ankle varus deformity of approximately 40° (Figure 1) was not fully correctable to neutral and he had persistent midfoot cavus due to a plantarflexed first ray (Figure 2). As a consequence of chronic lateral overload, painful callus had developed over the midfoot fifth metatarsal base. At the forefoot, there was elevation and clawing of all lesser toes and fixed dorsiflexion of the hallux.


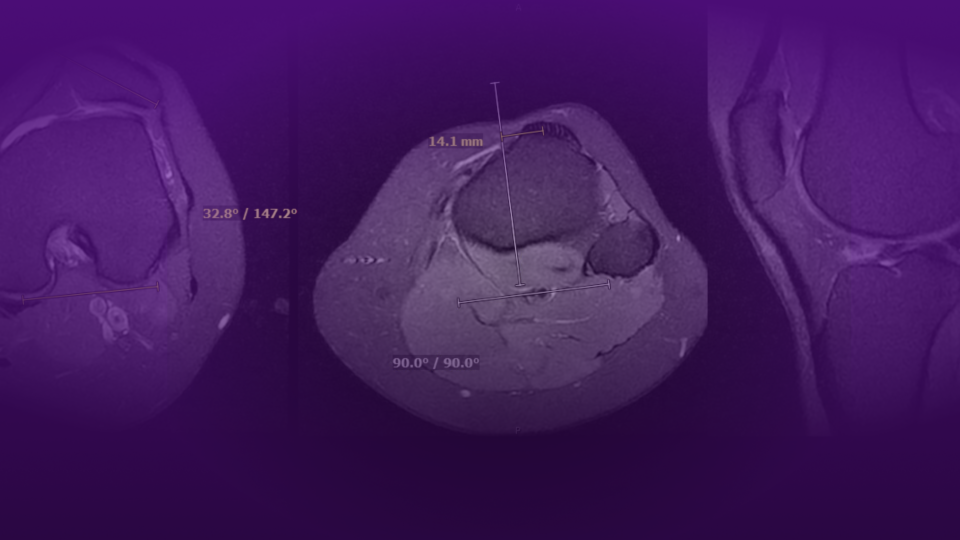
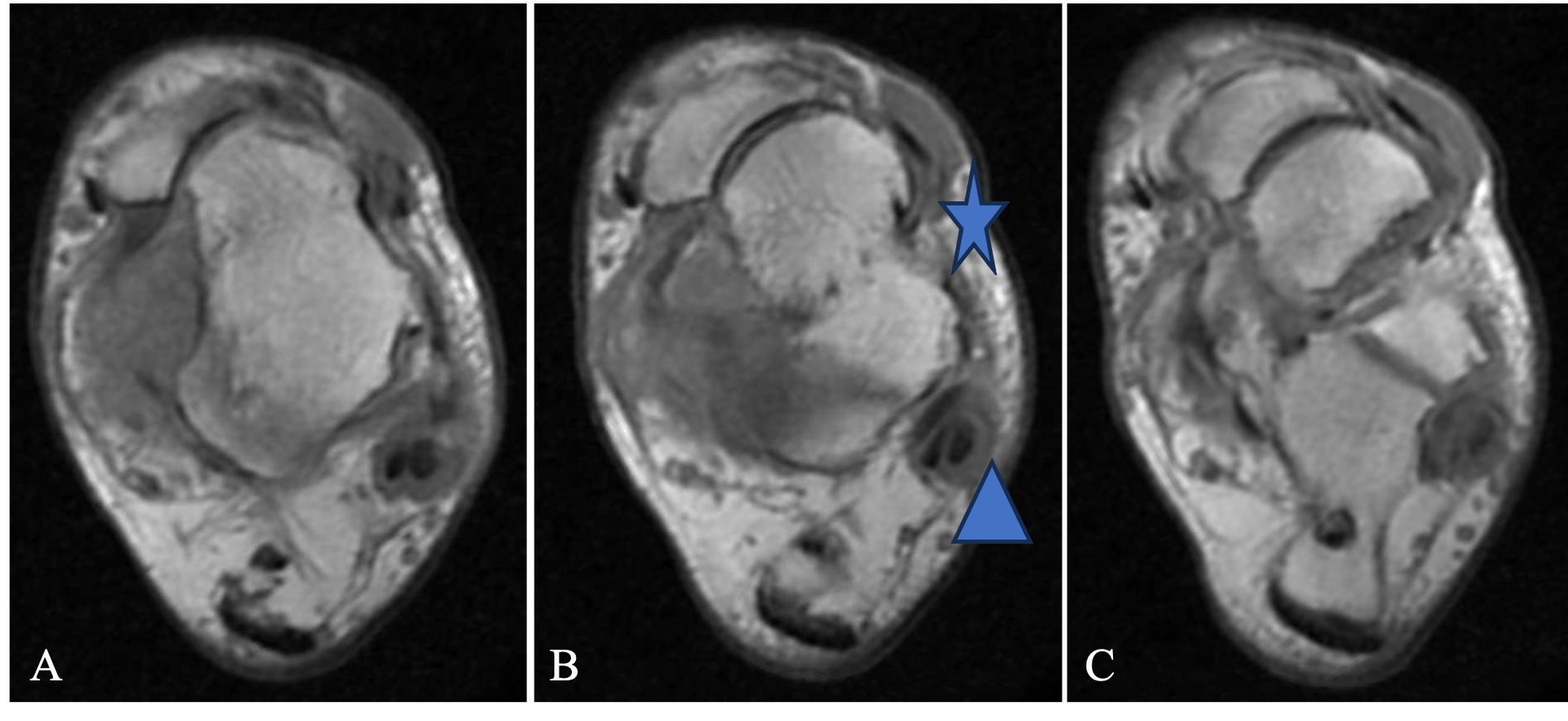
Plain film radiology of the ankle (Figure 3) confirmed significant ankle varus deformity with erosion of the medial tibial plafond and anterior subluxation of the talus. Foot X-rays demonstrated medial subluxation of the talonavicular joint consistent with clinical forefoot abduction, significant plantarflexion of the first ray and claw toe deformities. The preoperative weight-bearing CT also demonstrated subtalar instability with subluxation of the calcaneus medially (Figure 4). MRI confirmed deficiency of the lateral ligament complex and severe peroneus longus and brevis tendinopathy (Figure 5).


Operative Management
While two-stage surgery was considered, a single stage surgery, working in a proximal to distal approach permitted the painful pathologies to be addressed in one sitting and limit extended postoperative rehabilitation (Table 1).
Table 1. Procedures performed to address complex varus ankle arthritis and fixed cavovarus deformity in this case
| PROCEDURE | |
|---|---|
| 1 | Complex total ankle replacement with a modular stemmed system |
| 2 | Midfoot release with lengthening of the contracted tibialis posterior tendon |
| 3 | Achilles tendon lengthening |
| 4 | Subtalar fusion |
| 5 | Calcaneus lateral closing wedge & lateralizing osteotomy |
| 6 | Lateral column shortening through calcaneocuboid fusion |
| 7 | First metatarsal dorsiflexion osteotomy |
| 8 | Reconstruction of the lateral ligament complex |
| 9 | Peroneus longus to brevis tendon transfer and repair of the torn peroneus brevis tendon |
After administration of a combined saphenous and popliteal nerve block, the patient was positioned supine with a bump under the ipsilateral buttock. In severe ankle varus deformities, it is typically necessary to internally rotate the extremity at the hip to compensate for the external rotation at the ankle. We recommend obtaining a true mortise view using fluoroscopy prior to draping to confirm adequate positioning.
A standard anterior longitudinal midline approach was utilized. In varus ankles, the interval between extensor hallucis longus and extensor digitorum longus is sometimes necessary to ensure appropriate exposure of the lateral gutter. To correct the ankle varus deformity, it was necessary to perform a medial midfoot release at the talonavicular joint including the tibio-spring ligament, release of the superficial deltoid ligament, and fractional lengthening of the tibialis posterior tendon. A standard technique was then utilized for a stemmed total ankle replacement using the In-Bone System (Stryker).
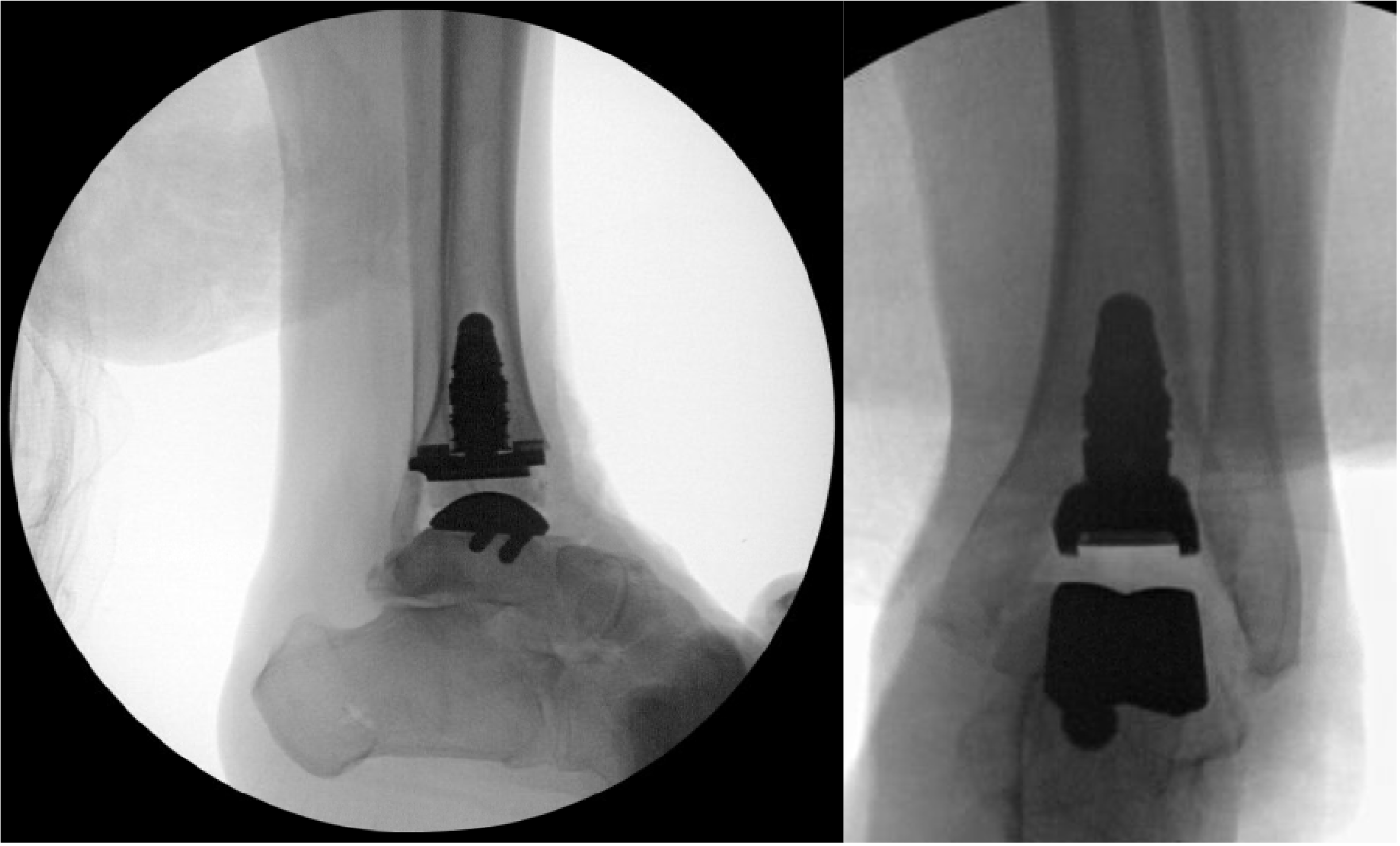
During trialing for the polyethylene, imbalance between dorsiflexion and plantarflexion confirmed requirement for a formal posterior ankle capsule release. Through a previous posteromedial incision, Z-lengthening of the Achilles tendon was performed combined with posterior ankle capsule release. Abundant scar contracture from previous surgery was resected. Definitive TAR implants were then inserted (Figure 6).
We then proceeded with hindfoot and midfoot deformity correction. A limited sinus tarsi approach was utilized to access and prepare the subtalar joint posterior facet for fusion. Formal debridement of the middle facet was not performed to prevent dissection under the talar neck and minimize compromise of talar vascular supply.
To achieve adequate hindfoot realignment, an additional calcaneal osteotomy was necessary. A separate posterolateral incision and approach was made to the calcaneal tuberosity ensuring an adequate skin bridge from the sinus tarsi incision. A lateral closing wedge osteotomy was combined with lateral translation. Combined fixation of the calcaneal osteotomy and the subtalar fusion was achieved with a 7 mm headless compression screw.
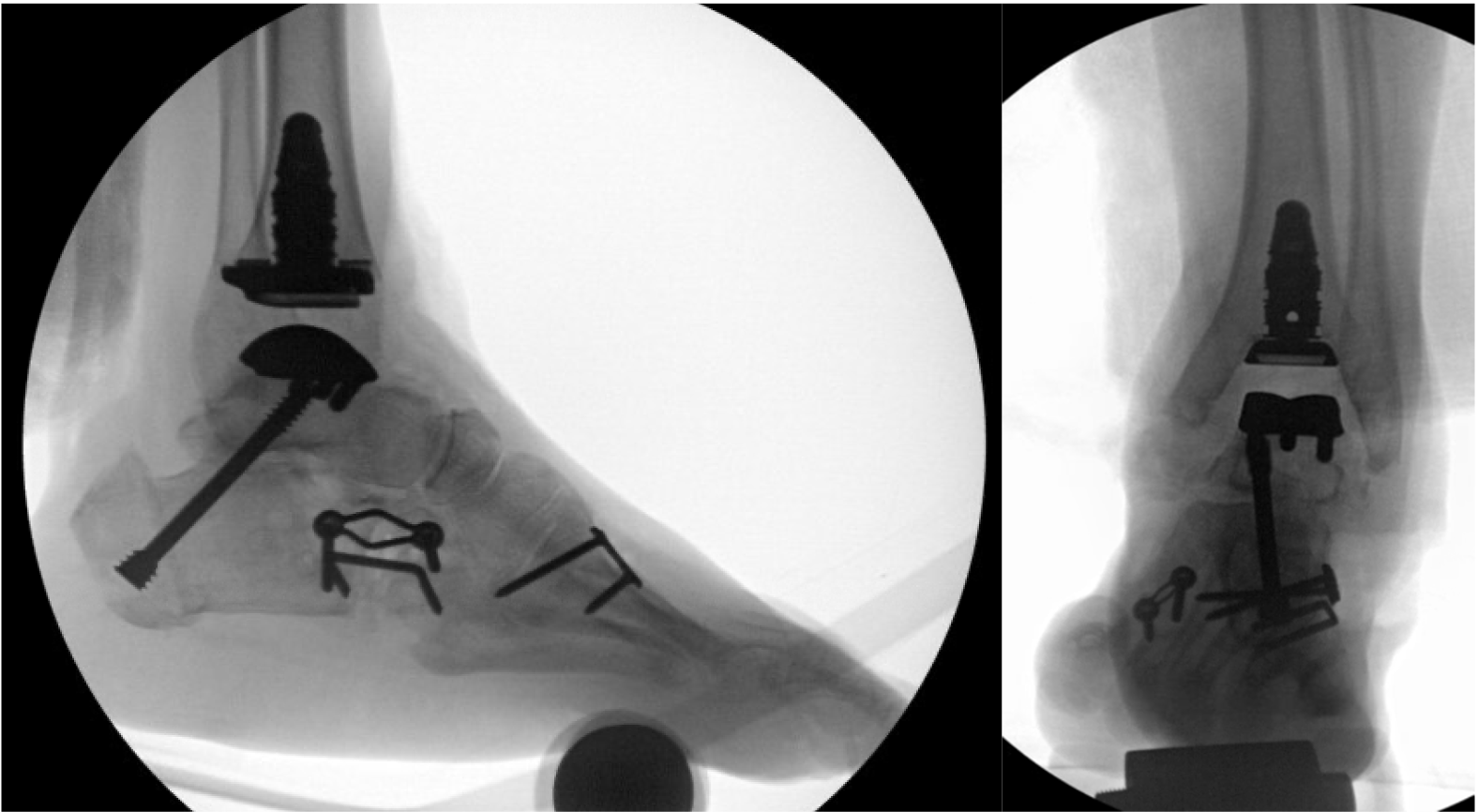
To address the forefoot supination and adduction deformities, flat-cut shortening osteotomies were performed at the calcaneocuboid joint through which a combination of lateral column shortening and midfoot de-rotation was achieved and fixed with a combination of a compression plate and staple. A dorsiflexion unicortical closing wedge osteotomy of the first metatarsal was achieved through a separate incision using a sagittal saw and fixed using a compression plate (Figure 7).
Ankle valgus stress examination confirmed persistent lateral ligament instability. The lateral sinus tarsi incision was curved proximally to the distal fibula. Secondary reconstruction of the lateral ligaments was achieved using a standard Brostrom-Gould procedure. Subsequent evaluation of the peroneal tendons demonstrated near-complete rupture of the peroneus longus and a complex tear of the peroneus brevis. Following debridement, the peroneus brevis was repaired with a running 3-0 vicryl suture. Peroneus longus tenotomy and transfer to brevis as a side-to-side tenodesis was performed to preserve its effect on ankle/hindfoot eversion. A prominent calcaneal peroneal tubercle was resected to prevent reinjury of the brevis tendon.
After extensive irrigation, layered closure was achieved with 3-0 vicryl to the deep fascia, subcutaneous tissues and basal dermal layer, and 4-0 nylon was used to approximate the skin without tension. A sterile soft dressing and well-padded splint were applied with the foot in neutral dorsiflexion.
Postoperative Course
At the two-week postoperative visit, all incisions were well healed with expected postoperative swelling and significantly improved alignment. Sutures were removed and the patient was maintained in a posterior splint non-weightbearing.
At the six-week follow-up, radiographs demonstrated maintained alignment, stable implant positioning, and progressive healing of the osteotomies and subtalar fusion. The patient transitioned to a controlled ankle motion (CAM) boot and began gradual protected weightbearing with initiation of formal physical therapy for ankle range of motion and strengthening.
At six months follow-up, the patient reported mild intermittent discomfort and was able to ambulate up to two miles per day. Examination demonstrated ankle range of motion of 10° dorsiflexion and 30° plantarflexion with stability to varus and valgus stress.
At the most recent follow-up two years postoperatively, the patient reported walking pain-free and was now able to go to the beach (Figure 8). Clinical examination demonstrated neutral foot and ankle alignment, pain-free ankle motion, and well-healed incisions. Radiographs demonstrated a well-positioned ankle prosthesis with complete healing of all fusions and osteotomies (Figure 9).


Discussion
Severe cavovarus deformity is a particularly challenging condition in patients with end-stage ankle arthritis due to the asymmetric loading of the tibiotalar joint and complex soft tissue disruption associated with malalignment.12 Historically, significant deformity was considered a relative contraindication to TAR given the higher rates of component loosening, polyethylene wear, and early implant failure.5,6 Advances in implant design and surgical techniques have expanded the indications for TAR in patients with complex deformities.
Trajkovski et al. reported that ankles with preoperative coronal deformities greater than 10° could achieve outcomes comparable to neutrally aligned ankles when ancillary procedures were performed to restore alignment and stability.5 Similarly, Lee and Lee demonstrated that TAR can be successfully performed in ankles with coronal plane deformities greater than 20°, with an implant survivorship of 92.3 percent at a mean follow-up of 74 months.9 Jung et al. reported successful outcomes in 10 ankles treated with TAR combined with calcaneal and metatarsal osteotomies for cavovarus deformity, with 90 percent patient satisfaction and significant improvements in pain and functional scores at early follow-up.15
The role of simultaneous subtalar fusion with TAR in the setting of cavovarus deformity has been established. Usuelli et al. demonstrated a 92 percent fusion rate with significant improvements in AOFAS scores (from 27.9 to 75.1) and ankle range of motion (from 12 to 32.8 degrees) at 12 months postoperatively.16 Recent data from Teehan et al. found that patients with simultaneous TAR and hindfoot fusions achieve meaningful clinical improvement and reach acceptable postoperative pain and function levels.17
This case demonstrates that even severe cavovarus deformity with end-stage ankle arthritis can be effectively treated with TAR when comprehensive deformity correction is undertaken. A combination of ligament balancing, tendon procedures, subtalar fusion, and multiplanar osteotomies can restore a stable, plantigrade foot with proper implant alignment, supporting the expanding role of TAR in complex deformities.
References
- Anastasio AT, Lau B, Adams S. J Am Acad Orthop Surg. 2024;32(16):738-746. DOI.
- Herrera-Pérez M, et al. J Clin Med. 2021;10(19):4489. DOI.
- Valderrabano V, et al. Clin Orthop Relat Res. 2009;467(7):1800-1806. DOI.
- Palmieri-Smith RM, et al. J Athl Train. 2017;52(6):610-623. DOI.
- Trajkovski T, et al. J Bone Joint Surg Am. 2013;95(15):1382-1388. DOI.
- Hanselman AE, Powell BD, Santrock RD. Orthopedics. 2015;38(4):e343-e346. DOI.
- Lee GW, Wang SH, Lee KB. J Bone Joint Surg Am. 2018;100(10):835-842. DOI.
- Queen RM, et al. J Bone Joint Surg Am. 2013;95(21):1927-1934. DOI.
- Lee GW, Lee KB. J Bone Joint Surg Am. 2019;101(24):2203-2211. DOI.
- Jung HG, et al. Foot Ankle Int. 2013;34(1):140-147. DOI.
- Adams SB, et al. Foot Ankle Int. 2020;41(3):259-266. DOI.
- Krause FG, et al. Foot Ankle Int. 2010;31(9):741-746. DOI.
- Johnson LG, et al. Foot Ankle Int. 2022;43(12):1622-1630. DOI.
- Jeng CL, et al. Foot Ankle Int. 2021;42(4):476-481. DOI.
- Jung HG, et al. Foot Ankle Int. 2013;34(1):140-147. DOI.
- Usuelli FG, et al. Foot Ankle Int. 2016;37(7):696-702. DOI.
- Teehan E, et al. Foot Ankle Int. 2025;46(8):845-854. DOI.