
Case Highlights:
- The creation of a neo-rectoperineal fistula with ultrasound guidance temporarily resolved a newborn’s imperforate anus.
- Progressive dilation of the neo-anorectal tract under fluoroscopic guidance allowed the baby to eat, defecate, and grow.
- After improvement of complicating omphalocele and cardiopulmonary conditions, a primary posterior sagittal anorectoplasty successfully reconstructed the baby’s anus.
A newborn presented to Hassenfeld Children’s Hospital at NYU Langone in February 2025 with an imperforate anus and a giant omphalocele that held his liver and intestines within a thin outward-bulging sac. The omphalocele, along with multiple other conditions including pulmonary hypoplasia and a large ventricular septal defect, greatly complicated the repair of his anorectal malformation.
Pediatric surgeon Laura Y. Martin, MD, explains that management of a giant omphalocele often follows a multi-stage “paint and wait” process: treating the sac to promote abdominal wall epithelization, waiting for the child to grow and accommodate a viscera reduction, and then reconstructing the abdominal wall. In newborns with an imperforate anus and no perineal fistula, meanwhile, “the intestines have nowhere to drain, so you have a dangerous blockage,” she says.
Surgeons typically perform a diverting colostomy to bring the colon to the abdominal wall, relieve the obstruction, and divert stool away from the urinary tract. However, due to the limited space available to create a diversion on the newborn’s abdominal wall, a lateral colostomy carried the risk of rupturing the omphalocele sac, interfering with pouching of the stoma, and complicating future abdominal wall reconstruction.
The alternative, a primary posterior sagittal anorectoplasty (PSARP), carried its own risks of early repair without a distal colostogram and limited abdominal access.
A Novel Percutaneous Approach
To resolve the complex case, Dr. Martin and pediatric surgeon Jason C. Fisher, MD, teamed up with pediatric interventional radiologist Frederic J. Bertino, MD, and pediatric surgery fellow Rachel Hanke, MD. After weighing the risks and benefits, the team opted for a third option suggested by Dr. Fisher: taking an ultrasound-guided percutaneous approach to relieve the obstruction via a neo-rectoperineal fistula.
“In this case, the approach became clear: adapting something routine for something innovative and lifesaving for this newborn.”
Frederic J. Bertino, MD
Dr. Bertino regularly performs transrectal aspirations and drain placements via a novel transabdominal sonographic window. After a discussion with Dr. Fisher, he agreed to try what amounted to a similar percutaneous procedure to create a fistula that could be dilated over time. “In this case, the approach became clear: adapting something routine for something innovative and lifesaving for this newborn,” he says.
The novel approach allowed the baby to eat, defecate, and grow until his improved cardiorespiratory function and epithelialized omphalocele significantly reduced the risk of the PSARP procedure. “We basically converted this complex situation into something similar to what we deal with every day,” Dr. Hanke says.
Lowering the Risk of an Anorectoplasty
In collaboration with Dr. Bertino, the team first localized the sphincter complex with electrostimulation and accessed the blind-ending rectum percutaneously with micropuncture under ultrasound guidance to ensure that nearby structures weren’t impacted. The team used the Seldinger technique to advance a guidewire through the baby’s rectal stump and into his meconium-filled rectum, and then place a Foley catheter through a peel-away sheath and create the neo-rectoperineal fistula.
“We basically converted this complex situation into something similar to what we deal with every day.”
Rachel Hanke, MD
Over a period of six weeks, the team progressively dilated the neo-anorectal tract under fluoroscopic guidance. “It was a nice combination of skill sets and we had regular conversations about when to safely upsize the tract and how to manage it exactly,” Dr. Bertino says. “So it was a good long-term collaboration.”
Six months later, after more skin had grown over the omphalocele and the baby’s cardiopulmonary conditions had stabilized, they performed a definitive PSARP procedure to reconstruct the baby’s anus, approaching it as they would have done for a naturally occurring rectourethral fistula.
Recovery and Outlook
At a follow-up visit three months after the PSARP, the baby was stooling with no issues and the care team was able to make plans to address his other comorbidities.
The case, Dr. Hanke says, illustrates how a close collaboration between pediatric surgery and interventional radiology yielded a creative solution in a challenging clinical scenario. “Because you have skilled physicians on both sides who are willing to think outside the box and push boundaries, it creates a place where new ideas can come to light,” she says. “We can also make sure we’re doing it in a safe fashion.”
“While we performed a unique procedure, he was a highly medically complex patient that benefitted from the expertise of an entire multidisciplinary team of neonatal experts.”
Laura Y. Martin, MD
Beyond the collaboration with interventional radiology, Dr. Martin emphasizes that resolving the case also relied on working closely with neonatology, cardiology, pulmonology, and ENT experts as well as occupational therapists to manage the patient’s overall care. “While we performed a unique procedure, he was a highly medically complex patient that benefitted from the expertise of an entire multidisciplinary team of neonatal experts,” she says.
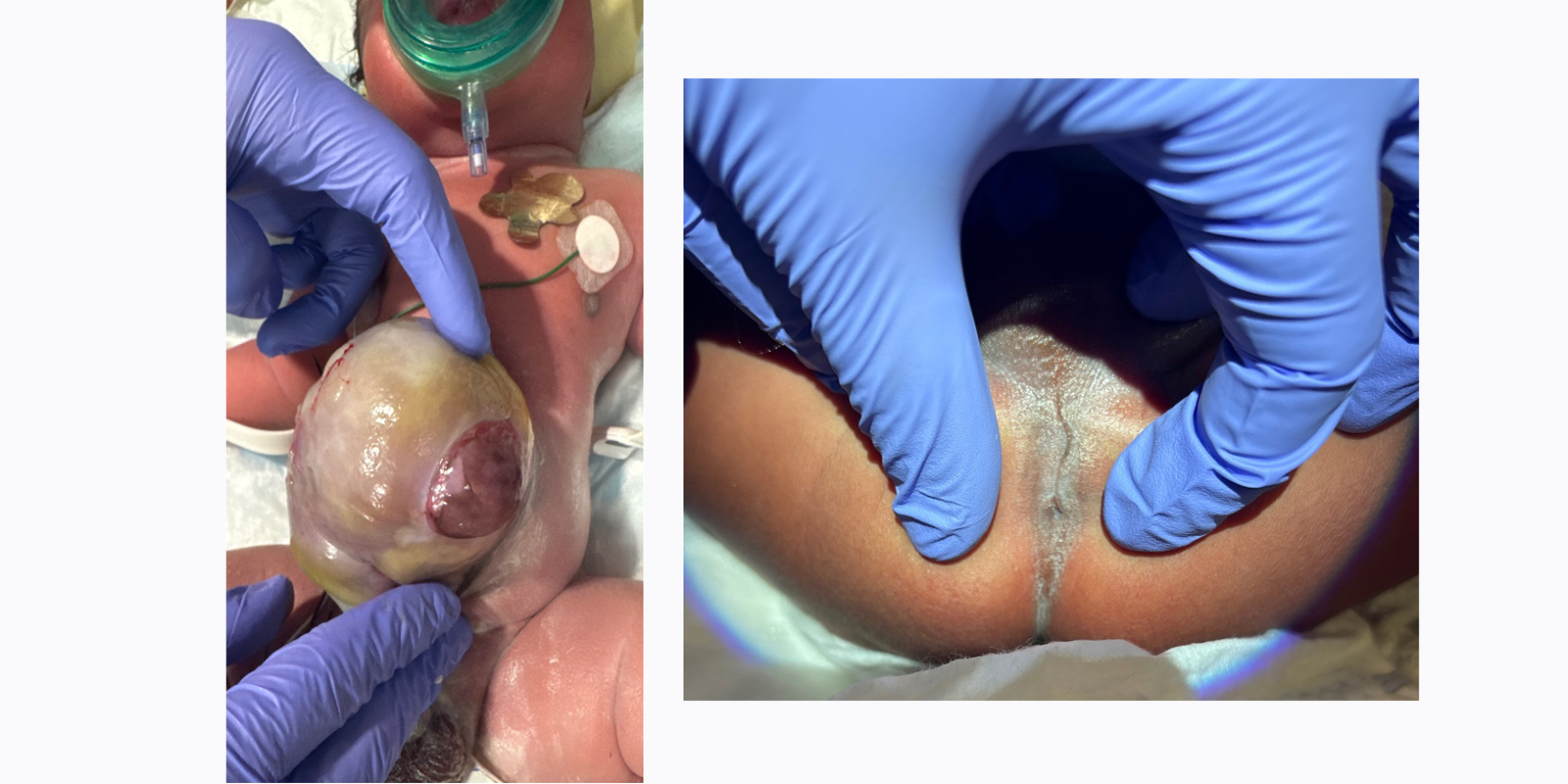
A full-term male baby was born with prenatally diagnosed giant omphalocele and an imperforate anus with no evidence of a perineal fistula. Source: NYU Langone Health.

Stimulating the sphincter complex allowed for percutaneous access with a micropuncture under ultrasound guidance. Source: NYU Langone Health.
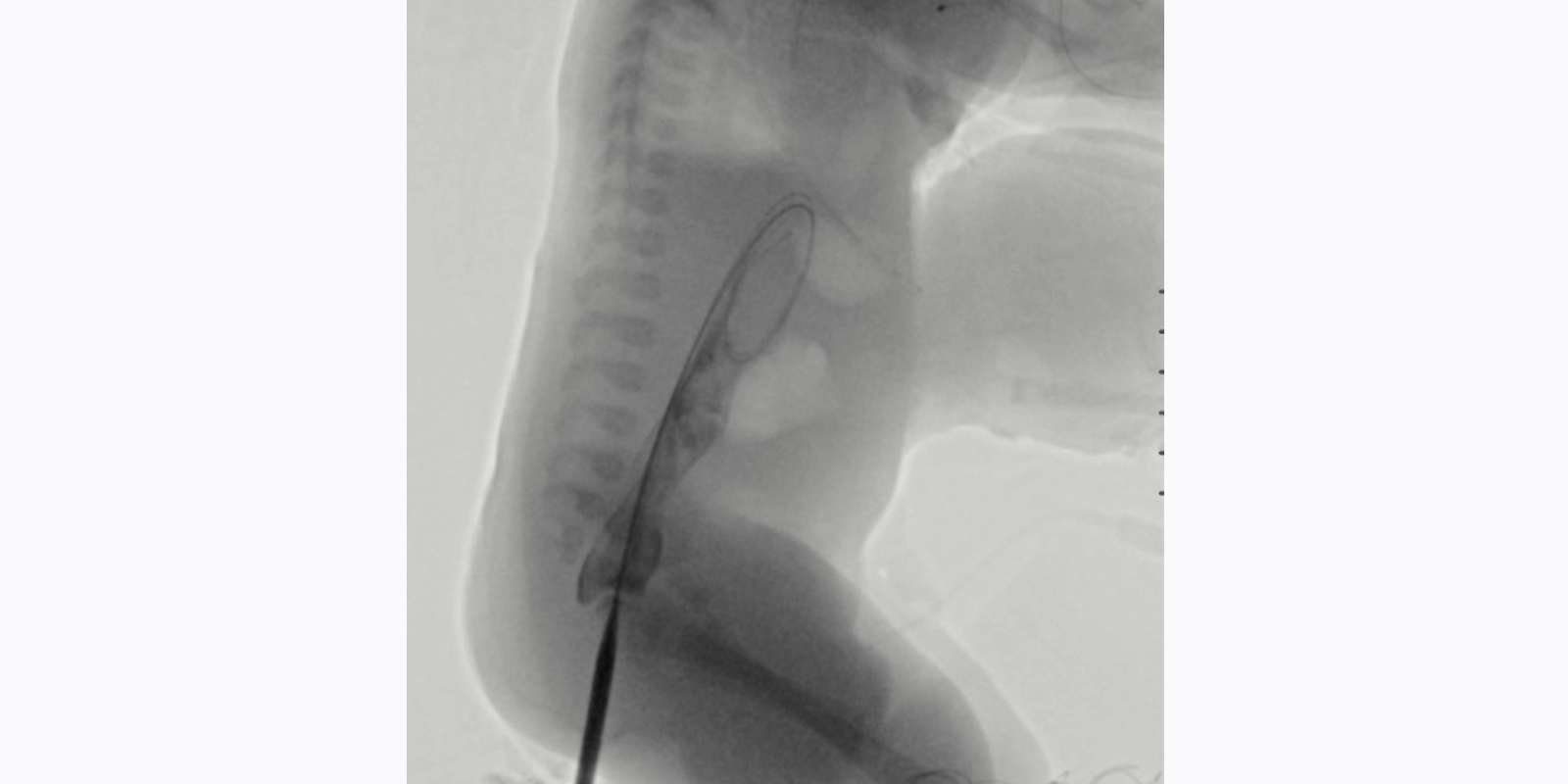
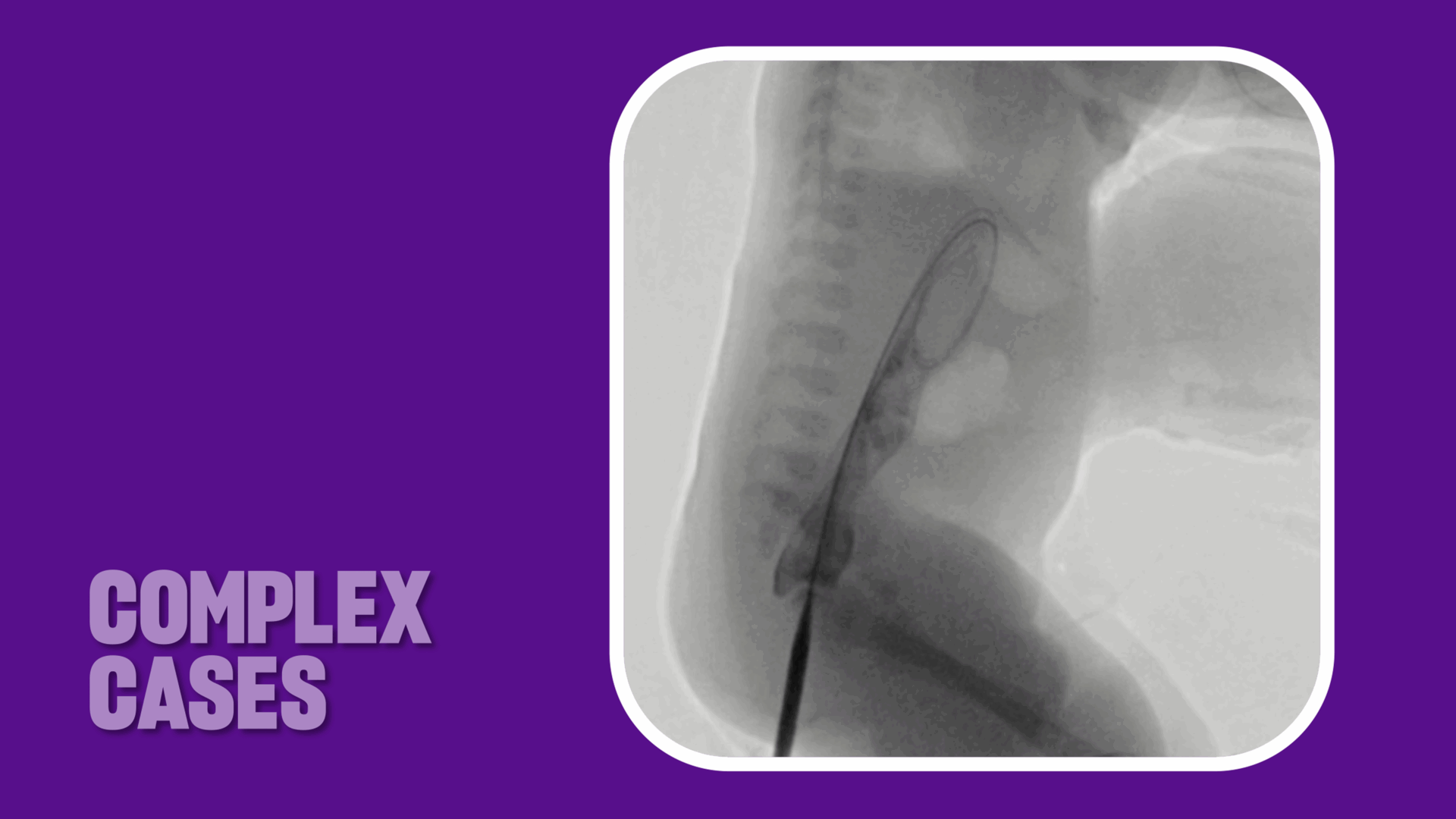
Inserting a stiff wire through the neo-anorectal tract allowed for serial dilation of the tract under fluoroscopic guidance. Source: NYU Langone Health.

Creation and progressive dilation of the neo-anorectal fistula significantly lowered the risk of a primary posterior sagittal anorectoplasty (PSARP), which was performed six months later. Source: NYU Langone Health.




