A healthy 34-year-old man presented with penile pain persisting for more than three weeks. The patient had been seen by two outside physicians for the same complaint prior to seeking my opinion.
The penile pain started a few hours after the man had had intercourse, which he characterized as “nothing out of the ordinary.” The pain was described as localized to the dorsal penile shaft, with tenderness and discomfort radiating from the midshaft dorsal to left lateral. A prominent vein on the dorsal penile shaft was identified as the area of maximal tenderness.
I noted the following observations during a physical exam and subsequently made the diagnosis of Mondor’s disease, involving a thrombophlebitis of the dorsal penile vein.
- Penis: Normal male phallus with normal urethra. No penile erythema or tenderness. No urethral discharge. A cord-like structure was palpable along the dorsal aspect of the penis that extended to the left lateral shaft. There was no hematoma, erythema, or signs of infection.
- Scrotum: No evidence of scrotal rashes.
- Testes: Nontender, with no swelling or masses bilaterally. There were no hernias or varicoceles, and the vas deferens and epididymis were palpable and normal bilaterally.
Here, I elaborate on the causes and clinical presentation of Mondor’s disease and detail the diagnostic workup. I also discuss management and the condition’s favorable prognosis.
Etiology and Clinical Presentation
A superficial vein thrombosis first described by Mondor in the chest wall in 1939, Mondor’s disease was broadened to include descriptions of penile phlebitis and thrombosis by Braun-Falco and Helm in 19581.
The incidence and prevalence of Mondor’s disease of the penis is relatively rare. Most existing literature is in the form of case reports describing potential etiological factors, such as trauma during sexual activity, vigorous masturbation, or penile infection. As in this patient, the most common presenting etiology is postcoital pain and discomfort, typically overlying a swollen and tender dorsal vein. The presentation of sudden onset of pain and a palpable cord-like structure along the dorsal aspect of the penis is common, but evaluation can be delayed by weeks in some situations.
Associated symptoms commonly include swelling, erythema, and bruising, noted especially when sexual activity is vigorous, causing trauma to underlying tissue. This is known as the so-called Virchow’s Triad of vessel wall damage: thrombophlebitis leading to venous stasis and subsequent clot formation2.
A thorough differential diagnosis for penile pain and discomfort should differentiate Mondor’s thrombophlebitis from other conditions like Peyronie’s disease or penile fractures. All three conditions can occur secondary to penile trauma, sustained most commonly while the penis is erect.
Diagnosis
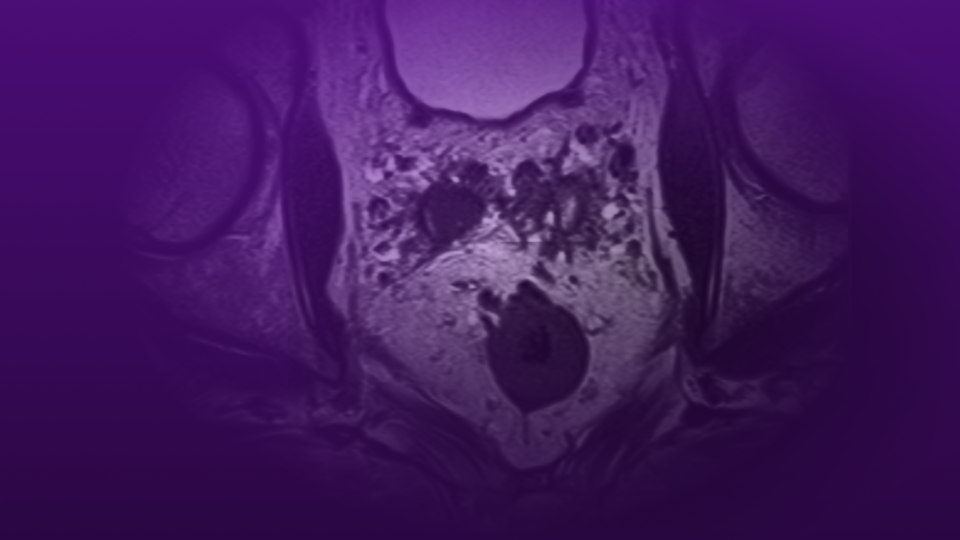
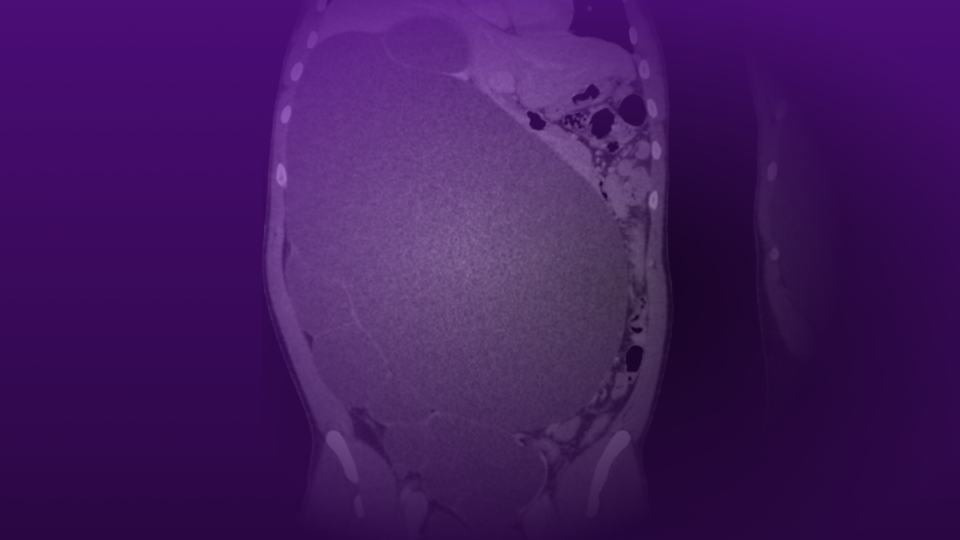
Diagnostic workup includes a thorough history and physical examination. When the presentation and physical exam are not straightforward, an imaging study is recommended. In our office, we have dedicated, urologically trained ultrasound technicians who have years of experience. An ultrasound is the quickest and least-expensive tool to diagnose Mondor’s disease. The characteristic findings of Mondor’s disease on ultrasound include a thrombosed vein, absence of arterial flow, and noncompressible vein consistent with thrombosis3.
More-detailed studies, such as an MRI of the genitals, can help to rule out penile fractures or other trauma-related penile injuries when ultrasound is not readily available or is inconclusive.
Management and Prognosis
Mondor’s disease of the penis is rare and is typically related to trauma during the erect state. Rarely do men with the condition need anything more than reassurance, anti-inflammatories, and behavioral modification. Urologists should consider this diagnosis in patients presenting with penile pain and cord-like structures once Peyronie’s disease and penile fracture have been ruled out.
Men with Mondor’s disease are often anxious and uncomfortable, and should be reassured that the condition is self-limiting. Conservative management options range from pain management with anti-inflammatories to warm compresses overlying the injured vein. Second-line treatments may be necessary in situations where the patient remains uncomfortable after conservative management. Consideration of anticoagulation therapy to prevent thrombus extension may be warranted in select cases; this can be done in conjunction with the vascular service. Antibiotic therapy should be administered when cellulitis is suspected4. Tapered steroid dosing has been described to reduce swelling and discomfort, but is unlikely to change clot formation and resolution.
Mondor’s disease has a very favorable prognosis, and symptoms usually resolve within weeks. However, patients may be very distraught and bothered by the injury and may seek out surgical treatment. There are rare cases in which surgical intervention, such as vein stripping, may be necessary for persistent cases of Mondor’s thrombosis5.
Some potential complications include recurrence, persistent pain, and mild erectile dysfunction due to condition-related anxiety or psychological distress.
References
1. Bird et al. (1997). Traumatic thrombophlebitis of the superficial dorsal vein of the penis: An occupational hazard. Am J Emerg Med.DOI.
2. Griger et al. (2001). Penile Mondor’s disease in a 22-year-old man. J Am Osteopath Assoc. PubMed.
3. Khan et al. (1982). New perspectives in diagnosis and management of thrombophlebitis of the superficial dorsal vein of the penis. J Dermatol Surg Oncol. DOI.
4. Nazir et al. (2010). Thrombosis of the dorsal vein of the penis (Mondor’s disease): a case report and review of the literature. Indian J Urol. DOI.
5. Swierzewski et al. (1993). The management of penile Mondor’s phlebitis: superficial dorsal penile thrombosis. J. Urol. DOI.