The prevalence of uric acid stones is increasing in parallel with obesity rates. 1,2 In one study, uric acid stones represented 24 percent of the stone burden in obese patients, compared with 7 percent in non-obese individuals.3
In this Case of the Month, we report the successful medical management of three moderate-to-large uric acid stones in a patient with obesity. Although percutaneous nephrolithotomy and ureteroscopy were considered, both were declined due to procedural risks associated with the patient’s body habitus. Urinary alkalinization therapy was selected with careful consideration of the patient’s overall health status and current medications.
Case Highlights:
- The patient presented with incidentally discovered kidney stones and was asymptomatic; she had a BMI of 50.
- Non-contrast CT revealed three stones with low attenuation (344 HU) and a urine pH of 5.5 to 6.0 consistent with uric acid composition.
- Given normal-to-high serum potassium levels (4.9 mmol/L) and losartan use, a low potassium citrate supplement was initiated, with the dose increased from 15 to 30 mEq citrate twice a day at three months.
- At four and a half months, near-complete dissolution was achieved, and by six months, the stones had fully resolved.
Patient Case
A 70-year-old woman was referred for evaluation of incidentally discovered left renal stones. She was asymptomatic, with no flank pain or gross hematuria. Her medical history included class III obesity (BMI 50) and hypertension managed with losartan.
Non-contrast CT revealed mild left hydronephrosis, ureteropelvic junction stones measuring 15 x 7 x 14 mm and 9 x 9 mm, and a lower pole stone measuring 17 x 5 mm (Figure 1). The stones were not visible on CT scout or kidney, ureter, and bladder (KUB) X-ray, which could either be due to body habitus or uric acid composition.
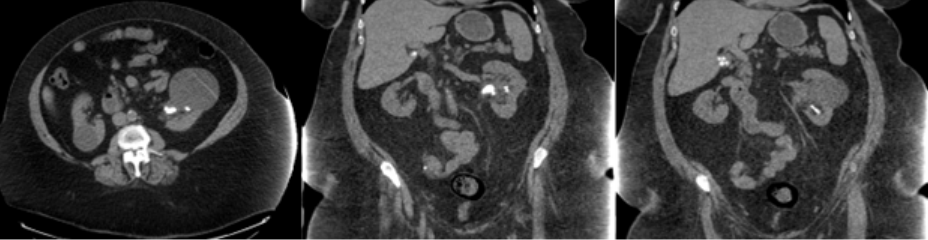
Stone density measured 344 Hounsfield units, and urine pH over the prior year ranged from 5.5 to 6.0—findings consistent with uric acid stone composition. Serum creatinine was normal and potassium was normal-to-high at 4.9 mmol/L.
Management
Given the moderate stone burden, percutaneous nephrolithotomy would typically be recommended. However, her body habitus posed technical challenges. Ureteroscopy was also considered, recognizing it might require two procedures to achieve complete stone clearance. As the patient remained asymptomatic, a trial of medical dissolution was pursued per her preference.
Urinary alkalinization is the cornerstone of uric acid stone management. While potassium citrate is standard, her elevated potassium and concurrent losartan use prompted selection of a lower-potassium alternative. She was started on Moonstone, an over-the-counter citrate supplement containing 5 to 7 milliequivalents (mEq) potassium per 30 mEq citrate. Initial dosing was 15 mEq (half packet) twice daily.
Follow-Up and Outcome
At three months, renal ultrasound showed reduced stone burden, though it was limited by body habitus. Urine pH remained at 6.0, prompting an increase in Moonstone to 30 mEq (one packet) twice daily.
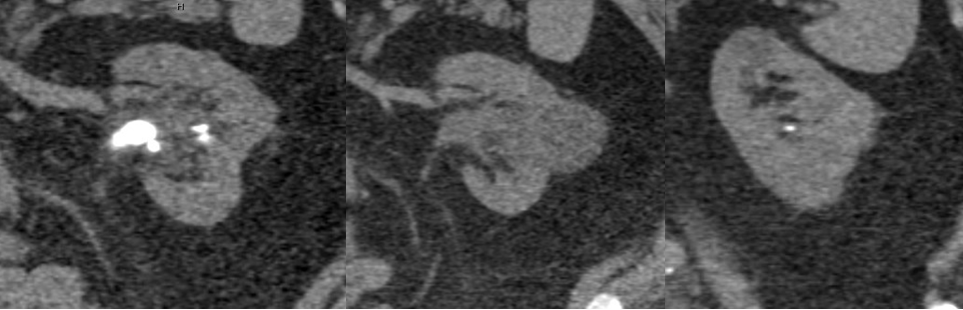
Six weeks later, repeat CT demonstrated near-complete resolution of all stones (Figure 2). Serum creatinine, potassium, and uric acid remained within normal limits. Six months later, an ultrasound showed no stones.
Discussion
Epidemiology and Pathophysiology
Uric acid stones account for about 10 percent of nephrolithiasis and affect approximately 1 percent of the general population.4,5,6 Risk factors include obesity, diabetes, gout, metabolic syndrome, and dehydration.7
Uric acid stones form primarily due to persistently low urine pH (< 5.5), which favors precipitation of undissociated uric acid. Hyperuricosuria may contribute but is less commonly the primary driver. American Urological Association (AUA) guidelines recommend urinary alkalinization to achieve a target pH of 6.0 to 6.5. Allopurinol may be added if alkalinization fails, primarily due to intestinal malabsorption disorders, or in cases of recurrent stone formation despite adequate alkalinization.
Certain medications—including losartan, NSAIDs, and vitamin C—can promote hyperuricosuria by inhibiting uric acid reabsorption within the kidney.
Diagnostic Considerations
Early recognition of uric acid stones is important and may obviate the need for surgical intervention in asymptomatic patients, as was demonstrated in this case. Urine pH ≤ 5.5 in a patient with nephrolithiasis should raise suspicion of a uric acid stone. Uric acid stones are radiolucent on KUB X-ray and often poorly visualized on CT scout images. On non-contrast CT, they typically exhibit low Hounsfield units (< 500). For stones > 4 mm, the combination of Hounsfield units ≤ 500 and urine pH ≤ 5.5 has a positive predictive value of 90 percent for uric acid composition.8
Prevention and Long-Term Management
Daily citrate therapy (Moonstone, potassium citrate, sodium citrate, or sodium bicarbonate) can prevent recurrence. Patients should aim for urine pH ≥ 6.0 at least once daily, measured two hours post-dose using pH strips.
Additional preventive strategies include adequate hydration to produce 2 to 2.5 L of urine per day, increased fruit and vegetable intake to boost urinary citrate and pH, and a low-purine diet to reduce uric acid production and acid load.9 Foods to avoid include red meat (beef, lamb, pork, venison), organ meats, poultry, shellfish and seafood, and high-fructose corn syrup.
References
- Xu LHR, et al. J Urol. 2017;197(6):1465-1471. DOI.
- Tran TVM, Maalouf NM. Curr Opin Nephrol Hypertens. 2020;29(4):407-413. DOI.
- Daudon M, Lacour B, Jungers P. Urol Res. 2006;34(3):193-199. DOI.
- Moses R, et al. Urolithiasis. 2015;43(2):135-139. DOI.
- Stamatelou KK, et al. Kidney Int. 2003;63(5):1817-1823. DOI.
- Scales CD Jr, et al. Eur Urol. 2012;62(1):160-165. DOI.
- Maalouf NM. J Ren Nutr. 2011;21(1):128-131. DOI.
- Spettel S, et al. Urology. 2013;82(1):22-26. DOI.
- Heilberg IP. Urolithiasis. 2016;44(1):57-63. DOI.