

In this Case of the Month, we present a man who experienced more than 20 years of excellent function following primary total hip arthroplasty (THA) before developing recurrent dislocations. Advanced EOS imaging revealed spinopelvic stiffness in a “stuck standing” pattern, altering the functional orientation of his hip components and predisposing him to instability. He subsequently underwent successfully revision THA. Notably, intraoperative assessment demonstrated that the original cemented femoral stem remained well fixed even after 24 years in situ.
The patient’s course illustrates decades of remarkable progress in THA, including the longevity of cemented femoral components, advances in highly cross-linked polyethylene (HXLPE), the role of advanced imaging in surgical planning, and the use of dual mobility (DM) constructs for dislocation prevention.
The case reinforces that, with continued innovation, achieving a lifelong hip replacement is within reach.
Case Highlights:
- A man in his 40s underwent primary left THA in 2001 with a Triology cup, Longevity HXLPE liner, CoCr femoral head, and VerSys Heritage cemented femoral stem.
- In 2024, 23 years later, he developed recurrent dislocations; sit-to-stand EOS imaging identified spinopelvic stiffness as a key contributor of instability, with a “stuck standing” pattern.
- During revision THA in 2025, the head and polyethylene liner were exchanged while the 24-year-old, still-well-fixed cemented femoral stem was retained.
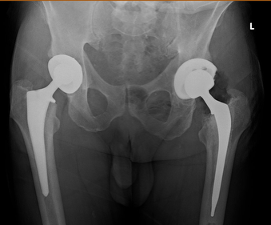
- During this period, the patient also underwent primary right THA, with DM technology used to mitigate dislocation risk.
Background: THA
THA remains one of the most successful surgical procedures for end-stage debilitating arthritis of the hip. Low friction arthroplasty of the hip, designed by Sir John Charnley in the 1960s, is one of the earliest successful hip arthroplasty designs, with data revealing 78 percent survivorship at 35 years.1,2 The hallmark design features of Charnley’s low friction hip include a cemented polyethylene liner, a 22-mm head, and a cemented femoral stem.
Since then, there have been significant improvements to the original design to address specific failure modes. For example, “cement disease” was later recognized to be caused by severe polyethylene wear. The resultant osteolysis has been addressed with both manufacturing modifications and processing improvements of polyethylene.3,4 One notable leap forward was the development of HXLPE, which has dramatically reduced wear rates and gives every hip replacement performed in 2026 a realistic chance of lasting a lifetime.5,6
Dislocation following THA remains one of the most common causes of revision surgery.7 DM technology represents a significant advancement in addressing instability, providing an increased effective head-to-neck ratio and a greater range of impingement-free motion.8,9
Further advances in THA stability have stemmed from an increased understanding of the lower lumbar spine dynamics on hip mobility. Stiff spine, defined as a change in sacral slope of less than 10 degrees between sitting and standing positions. “Stuck-standing” is defined as a sacral slope measurement greater than 30 degrees in both sitting and standing lumbar spine films, with a difference of less than 10 degrees. Alternatively, “Stuck-sitting” has been defined as a sacral slope measurement of less than 30 degrees in both sitting and standing lumbar spine films, with a difference of less than 10 degrees. These insights have provided new cup implant target zones to ensure hip stability.
Modern high-technology planning tools, including sit-to-stand EOS imaging and intraoperative navigation systems such as IntelliJoint, have enhanced the surgeon’s ability to optimize component positioning, particularly in the revision setting.10,11 Furthermore, advances in multimodal pain management, including regional anesthesia protocols and the routine use of tranexamic acid (TXA), have revolutionized rapid recovery and facilitated same-day discharge following THA.12,13
Patient Case
Initial Left THA. In 2001, a man in his early 40s presented with severe osteoarthritis of the left hip refractory to conservative management. Examination revealed an antlagic gait, pain with log roll, and a positive Stinchfield test. His left hip range of motion was extremely limited. Lower lumbar spine was non-tender to palpation at midline, free of stiffness or curvature.
He underwent primary left THA using a Longevity HXLPE liner, Trilogy acetabular cup, VerSys Heritage cemented femoral stem, and a 28-mm CoCr alloy femoral head (Figure 1). The postoperative course was unremarkable after a five-day hospital stay.
The patient reported complete pain relief at six weeks, shed the cane at one month with return to work, and full functional activity at eight weeks. He remained pain-free and fully functional for over two decades.

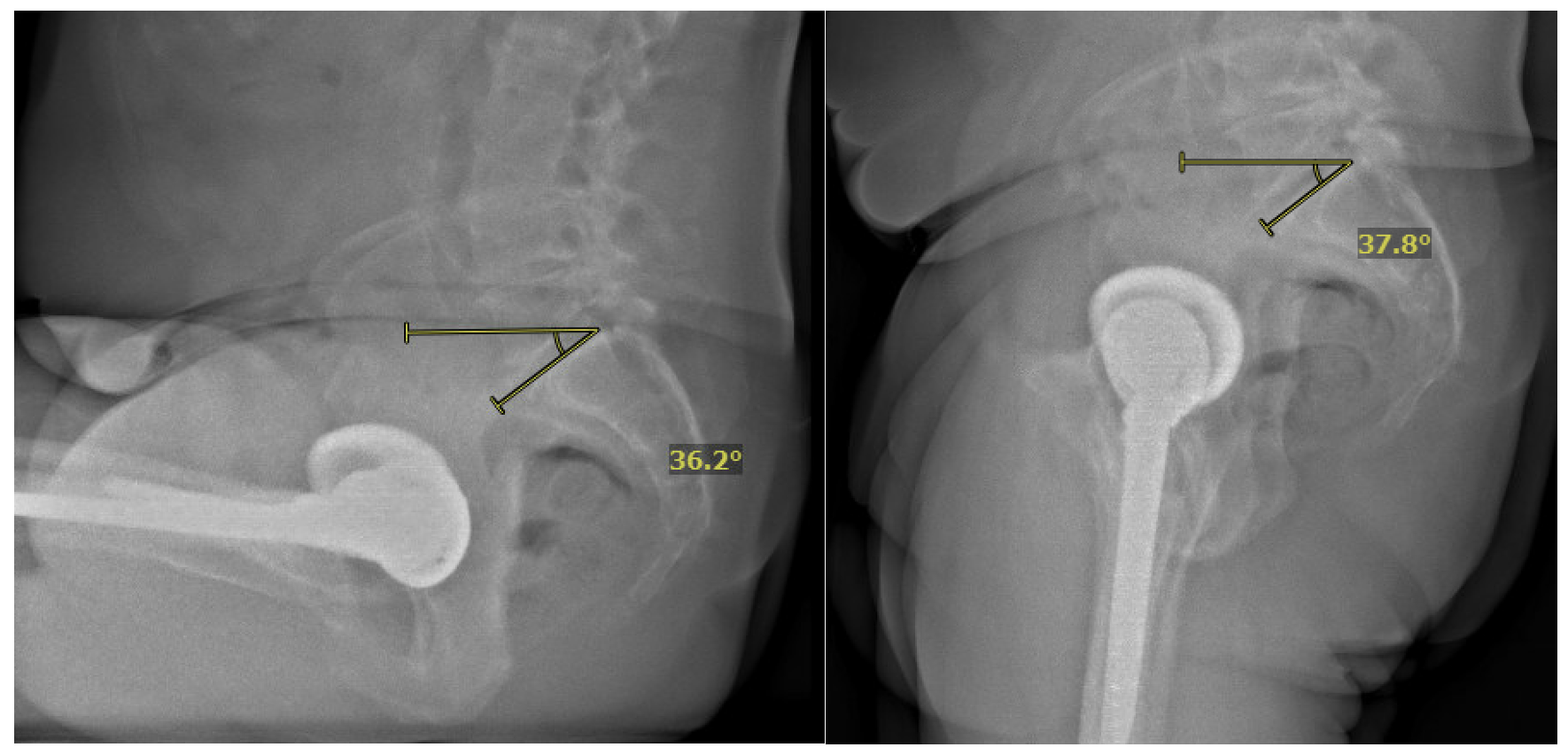
Left Hip Instability. In 2024, approximately 23 years after his index surgery, the patient began experiencing recurrent dislocations of his left hip. Evaluation included a sit-to-stand EOS scan, which revealed that his spine had become extremely stiff in a “stuck standing” position (Figure 2). This spinopelvic imbalance was identified as a significant contributing factor to the instability, as the restricted spinal motion produced unfavorable changes in pelvic tilt and, consequently, the functional orientation of the acetabular component during postural transitions.14
Subluxation episodes were precipitated by activities such as backpedaling during pickleball. This eventually grew into a frank dislocation event on the pickleball court which required closed reduction after sedation in an ED. We knew from the EOS planning that the patient was impinging (prosthetic neck on poly liner) posteriorly and coming out the front.
IntelliJoint navigation was made available as an intraoperative navigation to guide component positioning if cup revision became necessary. The decision was made to proceed with an isolated head and liner revision as the initial intervention, with preparation to revise the acetabular shell and adjust anteversion if mechanical impingement was not resolved.
Operative Management
In 2025, revision of the left hip was performed through the previous posterior approach. Intraoperative polyethylene wear pattern revealed evidence of mechanical impingement, posteriorly. Impingement was occurring at 10 degrees of left hip extension. The head and polyethylene liner were exchanged with a size 40 mm Biolox Delta ceramic head and a 40 mm ID / 64 mm OD XLPE liner. No posterior impingement was occurring past 25 degrees of hip extension. Importantly, the VerSys Heritage cemented femoral stem, now 24 years in situ, was well-fixed with excellent cement mantle integrity and was retained (Figure 3).
IntelliJoint navigation was available intraoperatively to assess component positioning and, if necessary, guide acetabular shell revision with adjusted anteversion.
Following the head and liner exchange, the construct was stable throughout a full range of motion, and mechanical impingement was resolved. The patient recovered in the postoperative anesthesia care unit and was discharged same day. He had an uneventful postoperative course.
To date, the patient’s mechanical impingement resolved and he has had no further dislocation events. The cemented VerSys Heritage femoral stem continues to demonstrate stable fixation at 24 years postoperatively, with intact cement mantle and no evidence of loosening or osteolysis.
Discussion
This case illustrates several converging themes in contemporary THA and highlights the remarkable evolution of the field over a single patient’s treatment course spanning more than two decades.
Longevity of Cemented Femoral Components. The cemented femoral stem, conceived by Sir John Charnley in the 1960s, continues to demonstrate an excellent track record. In this patient, the cemented stem has provided stable, pain-free fixation for 24 years with no evidence of loosening, subsidence, or periprosthetic osteolysis. This is consistent with registry data and long-term cohort studies demonstrating that well-cemented femoral components can survive three decades or longer.1,2,15 Notably, the stem was retained at the time of revision, requiring only a head and liner exchange, a testament to the enduring reliability of the cemented femoral fixation.
Advances in Highly Cross-Linked Polyethylene. The development of HXLPE represents one of the most impactful material advances in the history of arthroplasty. The original patient’s left hip was implanted with an early-generation highly cross-linked liner. Despite 24 years in situ, this bearing surface performed remarkably. Modern iterations of HXLPE, including vitamin E-stabilized and sequentially annealed formulations, have demonstrated even further reductions in wear, with projected wear rates so low that liner longevity may exceed the patient’s lifetime.5,6,16
Dual Mobility Technology and Dislocation Prevention. Dislocation remains a leading cause of revision after THA, with rates reported between 1 to 2 percent after primary surgery using a posterior approach.7,17 Dual mobility (DM) technology addresses this problem through a bipolar bearing design that provides a large effective head size and dramatically increases the arc of motion before impingement occurs. The senior author’s adoption of DM technology has resulted in a zero percent dislocation rate across more than 1,000 consecutive primary THAs over the past seven years, all performed through a posterior approach.
Advanced Planning in Revision Surgery. This case also demonstrates the value of modern preoperative and intraoperative planning tools in revision arthroplasty. Sit-to-stand EOS imaging identified the patient’s spinopelvic stiffness as a critical driver of instability, revealing a “stuck standing” pattern in which limited spinal flexion-extension resulted in inadequate posterior pelvic tilt during standing, effectively reducing functional acetabular anteversion.18
Multimodal Pain Management and Same-Day Discharge. The patient’s left revision THA was performed under a contemporary multimodal pain management protocol incorporating regional anesthesia and intravenous TXA. TXA has been shown to significantly reduce perioperative blood loss and transfusion rates, and its routine use has been a critical enabler of rapid recovery pathways and same-day discharge programs.19,20 The patient’s same-day discharge following his left revision THA exemplifies the modern rapid recovery paradigm, which integrates optimized anesthetic techniques, minimized surgical blood loss, and early mobilization.
Conclusion
This case demonstrates the convergence of decades of innovation in THA within a single patient’s treatment course. The enduring survivorship of a cemented femoral stem at 24 years, the evolution of polyethylene technology, the elimination of dislocation risk with dual mobility, the precision of modern planning tools in revision surgery, and the benefits of contemporary multimodal pain management collectively illustrate the remarkable progress in the field. As these technologies continue to mature, the expectation that a total hip replacement can last a lifetime is becoming an achievable reality.
References
- Berry DJ, et al. J Bone Joint Surg Am. 2002;84:171–177. DOI.
- Callaghan JJ, et al. J Bone Joint Surg Am. 2009;91:2617–2621. DOI.
- Harris WH. Clin Orthop Relat Res. 1995;311:46–53. Link.
- Dumbleton JH, Manley MT, Edidin AA. J Arthroplasty. 2002;17:649–661. DOI.
- Oral E, Muratoglu OK. Int Orthop. 2011;35:215–223. DOI.
- Kurtz SM, Gawel HA, Patel JD. Clin Orthop Relat Res. 2011;469:2262–2277. DOI.
- Bozic KJ, et al. J Bone Joint Surg Am. 2009;91:128–133. DOI.
- Darrith B, et al. Bone Joint J. 2018;100-B:11–19. DOI.
- Romagnoli M, et al. Int Orthop. 2019;43:1071–1082. DOI.
- Pierrepont J, et al. Bone Joint J. 2017;99-B:184–191. DOI.
- Pang M, et al. Arthroplast Today. 2024;30:101508. DOI.
- Scully RD, et al. J Am Acad Orthop Surg. 2020;28:E900–E909. DOI.
- Fillingham YA, et al. J Arthroplasty. 2018;33:3065–3069. DOI.
- Heckmann N, et al. J Bone Joint Surg Am. 2018;100:1845–1853. DOI.
- Morshed S, et al. Acta Orthop. 2007;78:315–326. DOI.
- McKellop H, et al. J Orthop Res. 1999;17:157–167. DOI.
- Wetters NG, et al. Clin Orthop Relat Res. 2013;471:410–416. DOI.
- Stefl M, et al. Bone Joint J. 2017;99-B:37–45. DOI.
- Lin ZX, Woolf SK. Orthopedics. 2016;39:119–130. DOI.
- Tuttle JR, et al. J Arthroplasty. 2014;29:1512–1515. DOI.



