Referral Notes:
- CSF–venous fistulas, first described in 2014, represent roughly half of all cases of spontaneous spinal CSF leak seen across the NYU Langone system.
- Transvenous embolization is a new treatment, and specialists at NYU Langone have applied the technique to treat over 50 patients with CSF–venous fistulas.
- Misdiagnoses are common, requiring specialists to differentiate CSF–venous fistulas from Chiari malformation.
- Experience understanding spinal vascular anatomy is central to treatment, and NYU Langone’s Basic and Advanced Neuroendovascular ANAtomy (BANANA) Course offers in-person training.
Over 50 patients with cerebral spinal fluid (CSF)–venous fistulas have been treated at NYU Langone Health using transvenous embolization of spinal veins. Pioneered by specialists at Mayo Clinic in 2021, the endovascular therapy has proven highly effective for CSF leaks caused by CSF–venous fistulas, offering an alternative to spinal surgery, the previous mainstay of treatment.
“We’ve been seeing more and more of these cases. They’re not that uncommon,” says neurointerventional radiologist Eytan Raz, MD, PhD, who has treated the majority of the center’s CSF–venous fistula cases. “The treatment is permanent for roughly 90 percent of patients, with approximately a 10 percent chance of the fistula recurring at another level.”
“We’ve been seeing more and more of these cases. They’re not that uncommon.”
Eytan Raz, MD, PhD
The learning curve for the endovascular treatment is not steep, explains Dr. Raz, and is safe, but some providers may be navigating a system they don’t usually navigate—spinal vein anatomy. What is more challenging, he says, is the diagnosis; patients often go through one to two misdiagnoses, causing unnecessary procedures.
A New Type of CSF Leak
First described in 2014, CSF–venous fistulas are now recognized as a leading cause of spontaneous CSF leak and intracranial hypotension, with the most common symptom being severe headache that worsens with standing, coughing, or straining.
The abnormal connection occurs between the spinal subarachnoid space and a nearby spinal vein, permitting CSF to flow directly into the venous system. The fistulas typically occur in the thoracic spine and sometimes in the lumbar region. The cause is unknown and they’re seen across all clinical contexts—affecting the young and old, male and female, healthy and sick alike.
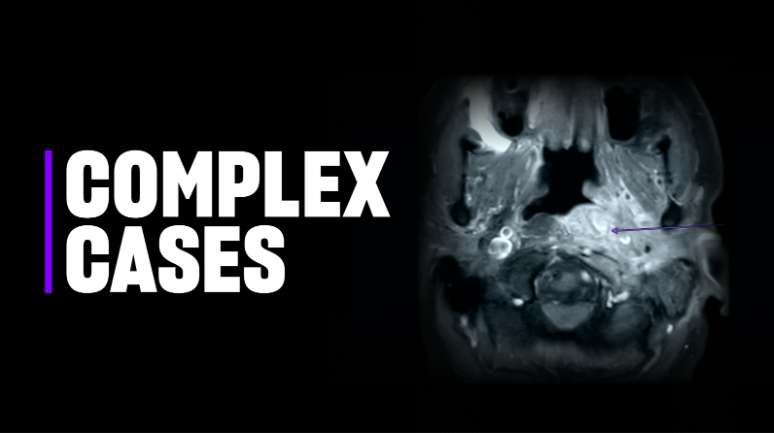
The detection and diagnosis of CSF–venous fistulas can be challenging. Unlike spinal CSF leaks from dural tears or a leaking nerve root sleeve, CSF–venous fistulas do not cause fluid to pool in the epidural space. As a result, the leak is not detected by a conventional spine MRI.
Instead, a brain MRI may detect changes indicative of CSF volume depletion, including meningeal enhancement and “brain sag,” or the downward displacement of the brain within the skull. Dynamic myelographic techniques are relied on to confirm the abnormal flow of CSF into a vein and pinpoint the leak’s location.
“This treatment is life-changing for patients, and that’s what we work for.”
At NYU Langone, lateral decubitus CT myelography is the specific imaging recommended when a CSF–venous fistula is suspected. To increase chances of detecting the leak, multiple CT acquisitions are performed, including immediately after the dye is injected and at later timepoints, and with the patient rotating between lying on their right and left sides.
Chiari malformation is one of the most common misdiagnoses of CSF–venous fistula, as headache and cerebellar tonsillar descent from CSF loss may be present in both conditions.
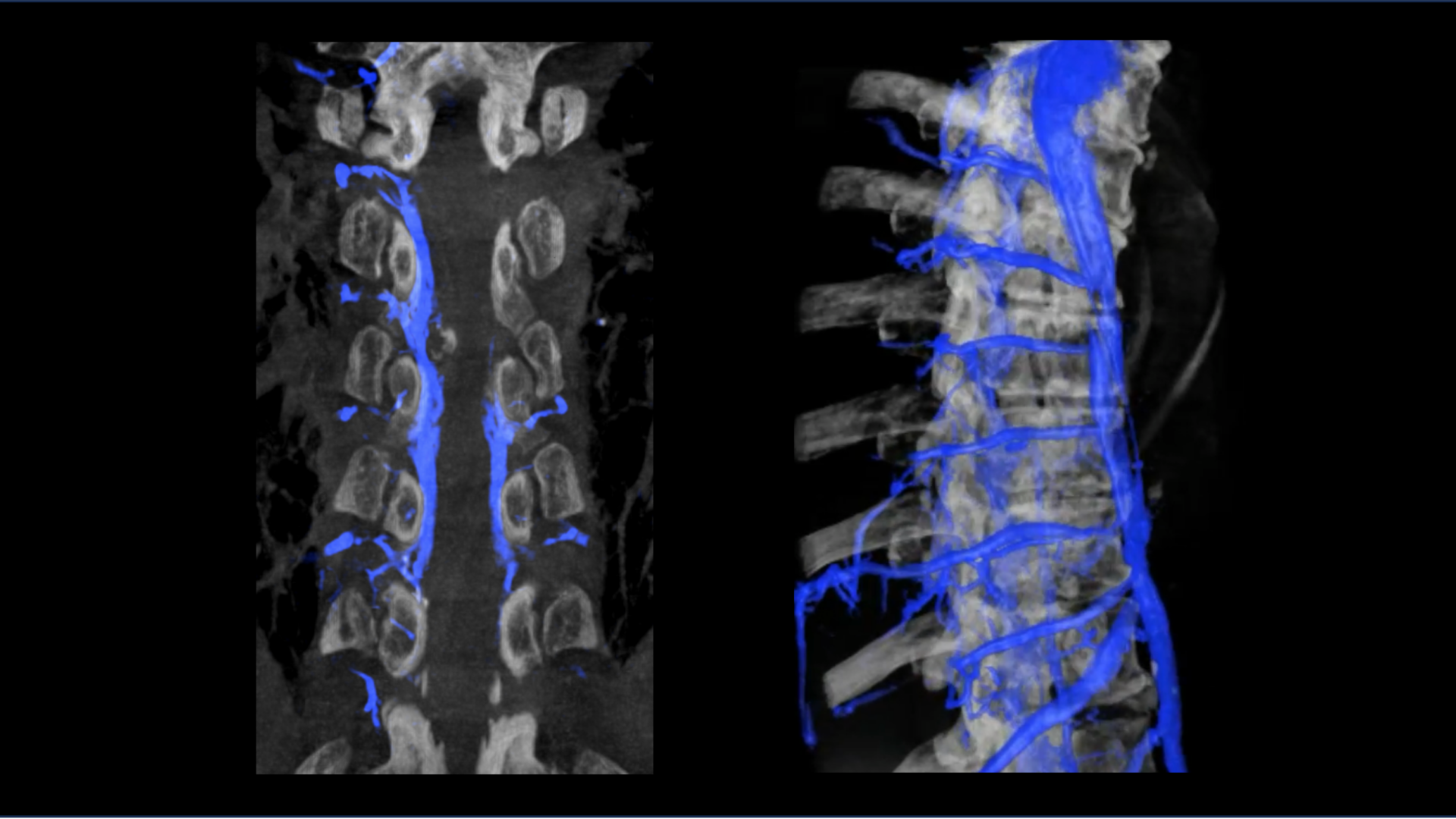
Navigating Paraspinal Veins
The general approach to the embolization is to gain access via the femoral vein and advance a catheter into the target paraspinal vein identified as draining the fistula. Roughly 1 to 2 mL of an embolic agent is slowly released. Fluoroscopic imaging is used to confirm that the embolic agent successfully occludes the pathway for CSF leak.
The procedure causes mild local pain at the site of embolization and patients can be discharged the same day. Most report symptom relief the next day.
To support training in this and other advanced vascular anatomy, NYU Langone offers a 3-day, in-person course—the Basic and Advanced Neuroendovascular ANAtomy (BANANA) Course—attended by specialists from across the globe.
“This treatment is life-changing for patients, and that’s what we work for,” says Dr. Raz. “To find a new group of patients that I can help with skills that I learned for something else—that is incredibly rewarding for me.”