Large renal stones in elderly patients are common and clinically challenging. While conservative management may be appropriate in selected asymptomatic, comorbid, or unwilling patients, it carries risks of renal deterioration, sepsis, and recurrent urinary tract infections (UTIs). When surgical intervention is pursued, management is often complicated by multiple comorbidities, chronic anticoagulation, and heightened thromboembolic risk. In this population, balancing effective stone clearance with procedural safety is paramount.
Percutaneous nephrolithotomy (PCNL) remains an effective option in older adults, including those on low-dose aspirin, however several studies suggest higher complication rates with advancing age.
Advances in ureteroscopy (URS)—particularly suction access sheaths, high-power thulium fiber laser (TFL) systems, and smaller ureteroscopes—have improved stone-free rates and reduced infectious complications, enabling treatment of larger stones in a single stage in select patients.
Here, we present the management of a large staghorn calculus in a woman in her 90s with recurrent infections, chronic anticoagulation, and multiple comorbidities, demonstrating how suction-assisted URS with TFL lithotripsy can achieve complete clearance in a single stage.
Case Highlights:
- The patient was managed conservatively for four years before developing recurrent UTIs and urosepsis, prompting reconsideration of intervention and election of URS.
- Use of a 12/14 Fr suction ureteral access sheath, 7.5 Fr flexible ureteroscope, and 200 um TFL enabled complete stone clearance in a single 2.5-hour procedure.
- Aspirin was continued and apixaban was held perioperatively.
- She had no postoperative complications and remained infection-free with stable imaging at six months.
Patient Case
A woman in her early 90s presented for evaluation of left staghorn renal stones and recurrent UTIs. Her comorbidities included atrial fibrillation on apixaban (Eliquis), prior stroke, coronary artery disease status post stents on aspirin, aortic stenosis status post transcatheter aortic valve replacement, papillary thyroid cancer status post partial lobectomy, lymphedema, breast cancer, hyperlipidemia, and sarcoidosis. She declines blood products for religious reasons.
She initially presented to our clinic in 2021 with hematuria associated with a Proteus UTI. Apart from hematuria, she had no infectious symptoms. CT imaging revealed a large left staghorn calculus. She was counseled on treatment options but preferred observation because she was asymptomatic and wished to avoid procedures.
She remained under surveillance for four years with minimal issues. Annual ultrasounds showed stable stone burden with very mild dilation of the left upper pole. Renal function remained stable, she reported no bothersome flank pain, and although she had bacteriuria, she denied symptomatic infections.
In January 2025 she developed a symptomatic UTI treated by her primary care physician. She had another UTI in March 2025. In May 2025 she presented to the hospital with fever and sepsis secondary to a UTI, with similar mild dilation of the left upper pole. An on-call urologist placed a ureteral stent, after which she returned to our clinic to discuss management options.
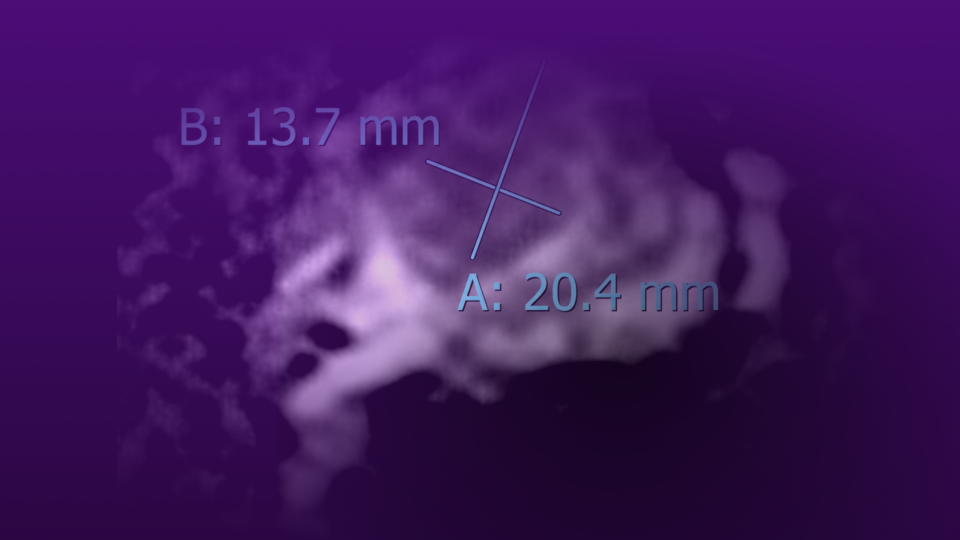
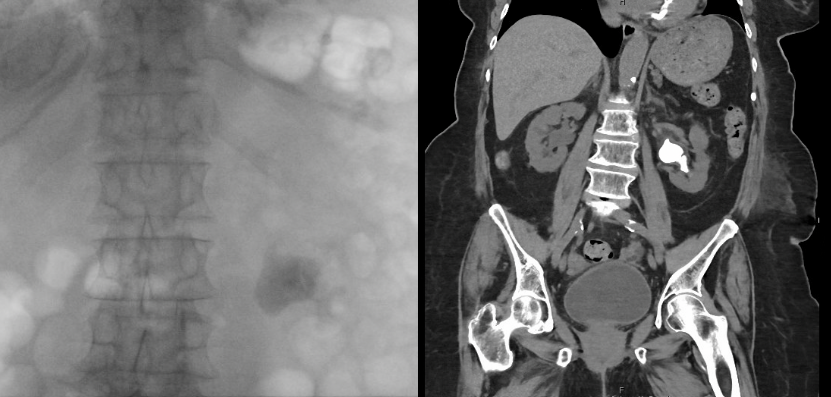
She presented with her children while completing a course of antibiotics and experiencing mild stent discomfort. She and her family preferred the least invasive option given her comorbidities, age, and religious beliefs, and sought to minimize bleeding risk as she declines transfusions. She required continued low-dose aspirin perioperatively but was able to temporarily hold apixaban for the procedure. After a detailed discussion of URS with laser lithotripsy, PCNL, and observation, the patient and family chose URS to address her recurrent infections and recent hospitalization. Preoperative imaging is shown in Figure 1.
Surgical Approach
In June 2025, two weeks after stent placement, she underwent left URS with laser lithotripsy and stent exchange. She was admitted preoperatively for 24 hours of intravenous antibiotics to decrease risk of infection. Apixaban was held perioperatively and low-dose aspirin was continued.
A 12/14 Fr flexible, navigable suction ureteral access sheath was placed without difficulty. A 7.5 Fr disposable flexible ureteroscope was used to evaluate the kidney, revealing a large staghorn stone. Lithotripsy was performed using a 200 μm TFL with dusting technique.
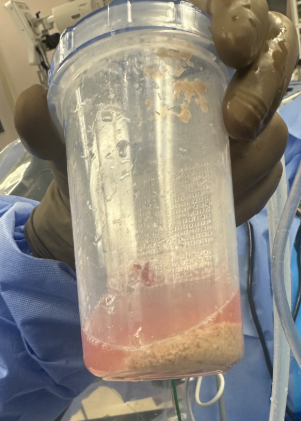
The stone was completely cleared. A large amount of dust was collected in the external stone collector attached to the access sheath (Figure 2). Most dust and small fragments were passively evacuated via suction during lasing; residual larger fragments were removed with a 1.9 Fr basket.
The procedure lasted approximately 2.5 hours, and the patient remained stable throughout. A ureteral stent was placed at the conclusion of the case.
Postoperative Care
She resumed apixaban the day after surgery. One week later her stent was removed without issue. At one month, ultrasound demonstrated a few tiny residual fragments and no hydronephrosis. At six months, she remained well with no interval infections and stable imaging.
Discussion
Nephrolithiasis is common, affecting about 12 percent of the global population, with prevalence increasing with age.1 Among patients older than 64 years, the rate of those undergoing definitive stone treatment increased from 67/100,000 to 89/100,000 between 1990 and 2010.2 Older adults often have multiple comorbidities, making definitive surgery more complex, and are more likely to be prescribed anticoagulants due to elevated thromboembolic risk.
Management of large staghorn calculi in elderly patients can be challenging. One important consideration is the safety of conservative management. A systematic review of seven retrospective studies of conservatively managed staghorn stones found mean rates of progressive renal deterioration of 27.5 percent, severe UTI of 8.7 percent, and recurrent UTIs of 50 percent.3 Our patient was managed conservatively for four years without significant issues until the onset of recurrent infections and a septic episode. While not ideal, conservative management may be reasonable in carefully selected, comorbid or unwilling patients with asymptomatic stones, with close monitoring.
The primary surgical options for large stone burdens are PCNL, URS with laser lithotripsy, and shockwave lithotripsy (SWL). In this case, the patient was counseled on PCNL and URS. She could hold apixaban temporarily but needed to continue low-dose aspirin. She declined PCNL due to the perceived increased bleeding risk and her refusal of transfusions.
Percutaneous Nephrolithotomy. PCNL can be effective in elderly patients. A recent review of PCNL in elderly patients reported no differences between elderly and younger patients in operative time (seven studies), stone-free rates (six studies), or retreatment rates (four studies).4 PCNL has also been performed safely in patients continuing low-dose aspirin; in one retrospective review (67 on aspirin vs 207 not on aspirin), there were no differences in residual stone, major complications (10.4 vs 5.8 percent, p=0.193), bleeding complications (3.0 vs 2.9 percent, p=0.971), or transfusion rate (1.5 vs 1.0 percent, p=0.57).5
However, several series suggest higher complication rates with advancing age. In a retrospective comparison of PCNL for complete staghorn stones, older patients had a statistically higher rate of minor complications (22.3 vs 41.9 percent, p=0.012) and a numerically higher rate of major complications (4.7 vs 12.2 percent, p=0.155).6
In another study comparing octogenarians with geriatric (60–79 years) and younger (20–59 years) cohorts, octogenarians had increased Clavien II–IV complications (28.8 vs 14.4 vs 10.4 percent, p=0.02) and higher transfusion rates (10.2 vs 4.7 vs 2.3 percent, p<0.001).7
Given these considerations, our patient declined PCNL.
Ureteroscopy. URS is first-line therapy for most stones under 2 cm. Over the last decade, there have been significant technological improvements in URS which have led to smaller scopes, higher-power lasers with improved dusting, and suction access sheaths. With these advancements URS has become increasingly popular in the elderly population. Studies on URS have shown high stone free rates and less complications compared to PCNL.8 URS for large stones may require staged procedures. In this case, the combination of a suction access sheath, TFL, and a small 7.5 Fr ureteroscope enabled complete clearance in a single stage.
Suction Access Sheaths. Suction ureteral access sheaths, introduced around 2015, modify traditional sheaths by adding a secondary channel at the distal end that connects to vacuum suction. These devices evacuate debris and dust during lithotripsy, improving visibility and stone clearance while maintaining low intrarenal pressures. Lower intrarenal pressure may mitigate complications such as patient discomfort, pyelovenous backflow, forniceal rupture, and sepsis. Newer sheaths include a bendable tip that can be passively deflected into different calyces by flexing the ureteroscope, improving access and clearance.
Preliminary data seem to show that suction action sheaths help improve stone free rates and decrease complications. An international multicenter randomized trial comparing suction versus traditional sheaths showed higher immediate and three-month stone-free rates, with lower overall complication and postoperative fever rates, and no differences in operative time, length of stay, or retreatment.9 Another study found lower rates of postoperative fever (5.5 vs 13.9 percent, p=0.009) and urosepsis (1.8 vs 6.7 percent, p=0.029) with suction sheaths.10
I have found in my own practice that suction sheaths work best when used in combination with a TFL system. This new laser technology allows for fine dusting which can be suctioned during the procedure. TFL, introduced clinically around 2018, has physical properties distinct from holmium:YAG that favor fine dusting: higher absorption coefficient in water, longer pulse duration, and lower peak power. In vitro studies show TFL produces more fragments under 0.5 mm and higher ablation rates compared to holmium at equivalent settings.11,12 Clinical studies have confirmed these laboratory findings with higher stone free rates and improved visibility during URS performed with TFL compared to holmium.13
Smaller-diameter ureteroscopes also enhance outcomes with suction sheaths by allowing more effective evacuation around the scope. Ideally, the scope’s diameter is at least 4–5 Fr smaller than the sheath’s outer diameter. In this case, a 7.5 Fr disposable ureteroscope paired well with a 12/14 Fr sheath. You could also use an 11/13 Fr sheath with the 7.5 Fr scope.
Together, these technologies have expanded the boundaries of stones amenable to URS. Stones over 2 cm, historically treated with PCNL, can often be managed ureteroscopically with suction-assisted dusting. Without suction, visualization during treatment of large stones can be compromised and residual fragments may lead to steinstrasse. With suction, dust can be continuously cleared, enabling safer and more reliable treatment of larger burdens. Our patient elected for URS and achieved an excellent outcome.
References
- Worcester EM, Coe FL. N Engl J Med. 2010;363(10):954-963. DOI.
- Ordon M, et al. J Urol. 2015;193(3):869-874. DOI.
- Alsawi M, et al. Ann R Coll Surg Engl. 2020;102(4):243-247. DOI.
- Schulz AE, et al. World J Urol. 2023;41(4):981-992. DOI.
- Otto BJ, et al. J Urol. 2018;199(3):748-753. DOI.
- Sahan M, et al. Cureus. 2021;13(11):e20001. DOI.
- Abedali ZA, et al. Urology. 2019;134:62-65. DOI.
- De S, et al. Eur Urol. 2015;67(1):125-137. DOI.
- Zhu W, et al. EClinicalMedicine. 2024;74:102724. DOI.
- Zhu Z, et al. World J Urol. 2019;37(5):921-929. DOI.
- Andreeva V, et al. World J Urol. 2020;38(2):497-503. DOI.
- Hardy LA, et al. Lasers Surg Med. 2019;51(6):522-530. DOI.
- Ulvik Ø, et al. Eur Urol. 2022;82(1):73-79. DOI.