In the spring of 2025, a female in her early 30s with severe pectus excavatum was referred to thoracic surgeon Costas Bizekis, MD for evaluation. Although the majority of patients with congenital pectus excavatum have corrective surgery in adolescence, the patient had delayed treatment due to insurance-related concerns.
The patient was reporting intermittent palpitations, chest pain, worsening shortness of breath with activity, and decreased exercise tolerance. “With a Haller Index of 6.5, the severity of the chest deformity was compressing the patient’s right atrium and ventricle, and limiting full lung expansion,” Dr. Bizekis says.
After carefully reviewing the patient’s chest CT imaging, he recommended the minimally invasive Nuss procedure.
“We’re among the few centers in the nation to offer an adult surgical pectus excavatum program.”
Costas Bizekis, MD
“We’re among the few centers in the nation to offer an adult surgical pectus excavatum program,” Dr. Bizekis says. He and colleagues at NYU Langone’s Department of Cardiothoracic Surgery focus on complex cases, emphasizing improved breathing and quality of life for adults with pectus excavatum and other congenital chest wall conditions.
Surgical Approach
Dr. Bizekis and team began the procedure with bilateral cryoablation of the third through eighth intercostal nerves on both sides. “Cryoablation helps mitigate postoperative pain and significantly impacts the patient’s ability to recover faster,” Dr. Bizekis says. “We can often get patients home in one day.”
Under thoracoscopic guidance, Dr. Bizekis performed the Nuss procedure via two bilateral, 3-centimeter lateral chest wall incisions. After freeing up tissue under the sternum with a handheld sound incision device, he inserted three U-shaped, malleable titanium bars using passers connected to a guiding rod, conforming the bars to the chest wall.
“We decide intraoperatively how many bars to use. Although one or two bars is common, we implanted three bars because of the severity of this case,” Dr. Bizekis says.
During the operation, the bars were positioned one interspace apart in a submuscular plane along the outer surface of the pectoralis muscle and inverted to remodel the anterior chest wall, achieving correction without tissue resection, dissection, or chest tube drainage. The bars were secured to the lateral chest wall with FiberWire sutures.
Postoperative Management
“Pectus excavatum with a high Haller Index and significant compression of the heart that required three bars isn’t common, but with the use of cryoablation and no chest tube drainage, the patient was able to go home the first post-operative day with an excellent result,” Dr. Bizekis says.
“With the use of cryoablation and no chest tube drainage, the patient was able to go home the first post-operative day.”
Dr. Bizekis saw the patient postoperatively at two weeks, one month, and three months, and will continue to see the patient annually for follow-up. The titanium bars will remain for three years before surgical removal as an outpatient procedure.
After one month of recovery, the patient was cleared to go back to the gym and reported increased physically active without shortness of breath. “Her exercise tolerance was much better and with a noticeable difference in appearance, she was extremely pleased with the outcome,” Dr. Bizekis says.
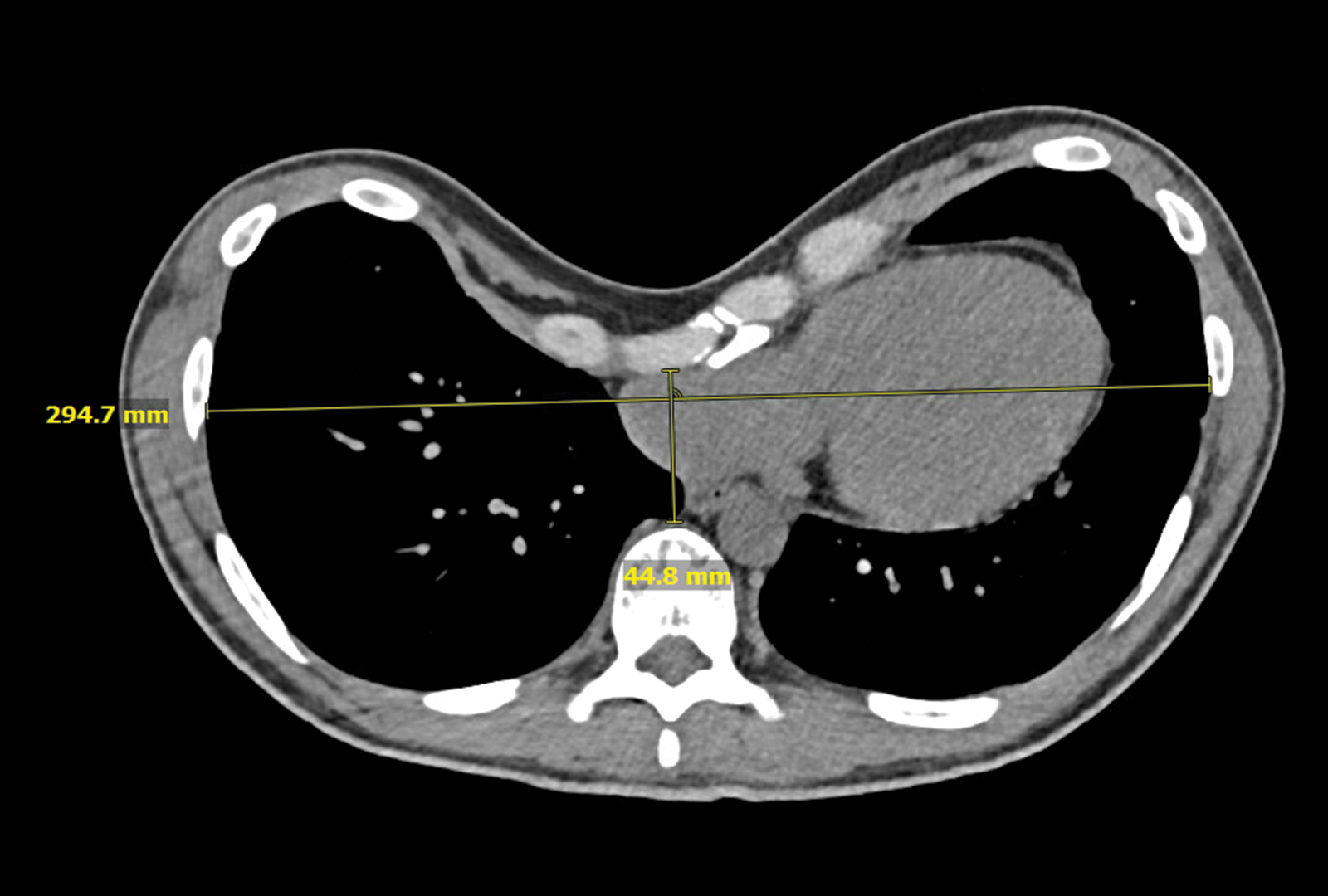
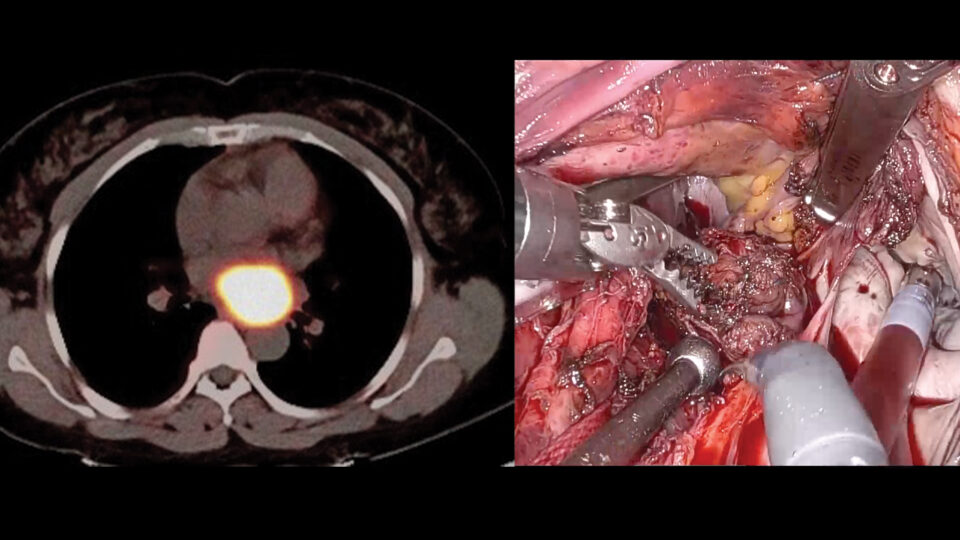
Preoperative chest CT of the patient’s pectus excavatum. Source: NYU Langone Health
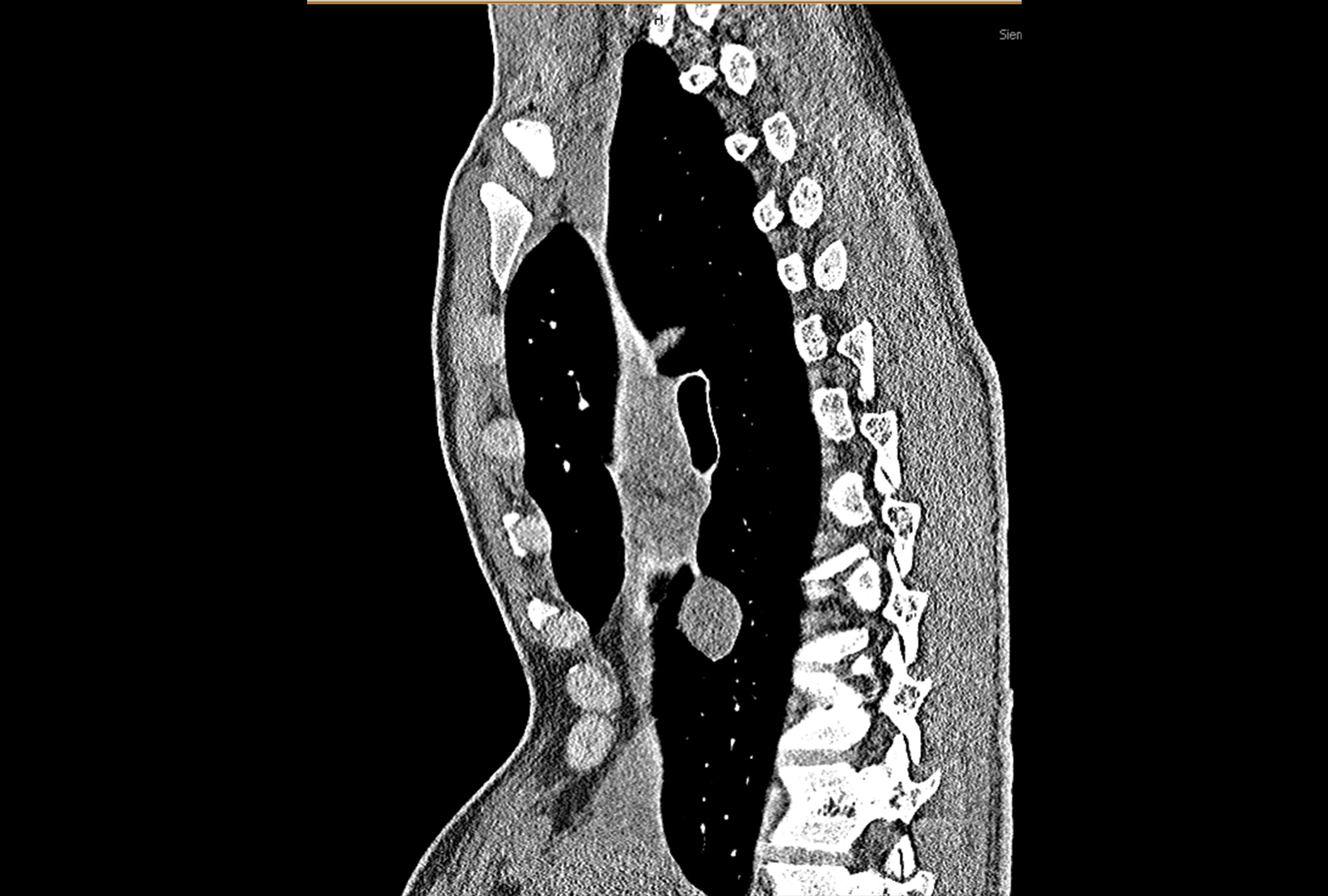
Sagittal view of the patient’s pectus excavatum. Source: NYU Langone Health

Postoperative X-ray showing placement of the three U-shaped titanium bars. Source: NYU Langone Health