When a 38-year-old male with a bicuspid aortic valve and a history of mitral valve endocarditis developed a rare complication—two massive pseudoaneurysms of the left ventricular outflow tract (LVOT)— specialists at NYU Langone Health’s Aortic Center devised a precise surgical plan to restore stability and function.
The patient’s cardiac history dated back to 2019, when he underwent a robotic mitral valve repair for endocarditis following a tooth extraction. In the years that followed, he remained active, exercising regularly without chest pain or breathing discomfort. However, in March 2024, a routine evaluation revealed moderate aortic insufficiency and an unusual aortic root finding that prompted his referral to the Aortic Center.
Cardiothoracic surgeon Mark D. Peterson, MD, PhD, system director of aortic surgery, evaluated the case. Based on initial transesophageal echocardiography, the finding was labeled a sinus of Valsalva aneurysm, but Dr. Peterson’s interpretation of CT angiography instead confirmed two large pseudoaneurysms—one measuring nearly 7 cm—along with a dilated aortic root and ascending aorta. Given the risk of rupture and worsening valve function, he recommended expedited surgical repair.
“The Ross procedure was discussed as a potential option for valve replacement, but we hoped his bicuspid valve would be repairable despite the size and location of the pseudoaneurysms.”
Mark D. Peterson, MD, PhD
“After reviewing his imaging, we planned a valve-sparing aortic root replacement, full ascending and hemiarch replacement, and patch repair of both pseudoaneurysms,” Dr. Peterson explains. “The Ross procedure was discussed as a potential option for valve replacement, but we hoped his bicuspid valve would be repairable despite the size and location of the pseudoaneurysms, particularly the one located both below and above the left coronary cusp.”
For younger patients, Dr. Peterson recommends the Ross procedure to avoid bioprosthetic valves, which carry a risk of early valve degeneration and reoperation. The patient strongly favored the Ross procedure or a bioprosthetic valve, eager to avoid a mechanical valve due to the requirement for lifelong anticoagulation.
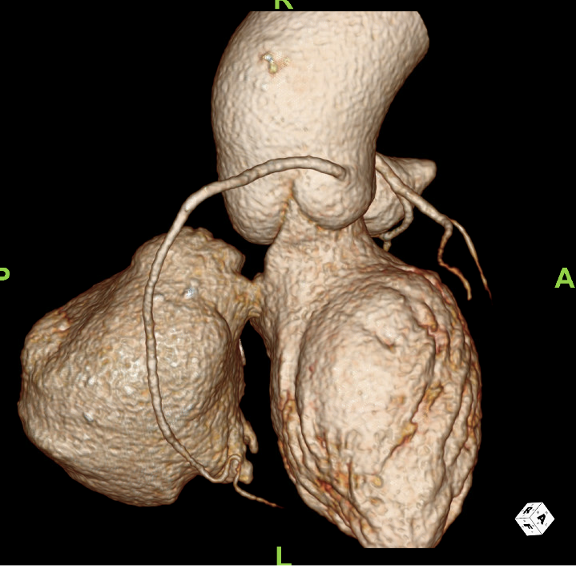
To aid the surgical team in preoperative planning, cardiac imaging specialist Puneet Bhatla, MD, and colleagues in radiology built a 3D reconstruction of the patient’s cardiac anatomy. During the surgery, Dr. Peterson and the team found that despite perforation at the base of the left coronary cusp as well as a hole below the cusp, the patient’s valve was salvageable.
As planned, they successfully patched and closed both pseudoaneurysms in the LVOT while performing the aortic root and hemiarch replacement. Cardiothoracic surgeon T.K. Susheel Kumar, MD, assisted with the procedure. Surgeon Michael P. Salna, MD, was recently recruited to the Aortic Center to contribute to the center’s growth.
Post-surgical echocardiography demonstrated normal left and right ventricular function, as well as a fully functioning aortic valve with no insufficiency. All other valves were functioning normally. The patient recovered uneventfully, was extubated in the operating room without complication, and was discharged on post-op day five.
Aortic Root Aneurysm

CT angiography revealing a 43 mm dilation of the patient’s aortic root and 53 mm ascending aorta. Source: NYU Langone Health
Ascending Aortic Aneurysm

CT angiography revealing a 53 mm dilation of the patient’s ascending aorta. Source: NYU Langone Health
First Pseudoaneurysm of the LVOT

Imaging also revealed a pseudoaneurysm of the LVOT under the annulus of the left sinus of Valsalva with contrast extravasation contained underneath the pulmonary artery. Source: NYU Langone Health
Second Large Pseudoaneurysm (View 1)
A second large pseudoaneurysm of the LVOT (measuring 66 x 69 mm) was found under the noncoronary sinus of Valsalva in the region of the ventricular septum. Source: NYU Langone Health
Second Large Pseudoaneurysm (View 2)

A second large pseudoaneurysm of the LVOT (measuring 66 x 69 mm) was found under the noncoronary sinus of Valsalva in the region of the ventricular septum. Source: NYU Langone Health