Just four days after undergoing a robotic Ivor Lewis esophagectomy to resect 60 percent of his esophagus, a 60-year-old man was discharged home—returning to work within just 10 days. His rapid recovery reflects NYU Langone Health’s depth of expertise with the fully robotic approach.
“We’re among the few centers in the world that performs this surgery with a completely robotic approach,” says thoracic surgeon Costas Bizekis, MD, whose team has completed hundreds of successful robotic-assisted Ivor Lewis esophagectomies over the past decade.
Surgical Approach
The patient presented with a history of GERD. Esophagogastroduodenoscopy with biopsy revealed a malignant tumor at the gastroesophageal junction, immediately treated with endoscopic submucosal dissection. Histopathology showed tumor invasion 1.5 mm into the submucosal layer, consistent with stage T1b adenocarcinoma, with possible lymphovascular invasion.
One month later, he underwent a robotic Ivor Lewis esophagectomy. Dr. Bizekis and his team guided the da Vinci’s articulating wrists to resect 60 percent of the patient’s esophagus, reconstruct a gastric conduit, and perform intrathoracic anastomosis—all accessed through four ports distributed across the patient’s abdomen.
Following the four-hour operation, the patient was discharged directly to the floor, bypassing the ICU, and was stable enough to go home in four days—less than half the typical nine-day length of stay reported for robotic cases, and well below the two-week average for open Ivor Lewis procedures. “The majority of our patients return home in four days, which is incredible,” Dr. Bizekis says.
Importantly, the patient experienced no complications, including anastomotic leak, which occurs in 5 to 10 percent of cases nationally, Dr. Bizekis says, regardless of whether surgery is performed in an open manner or robotically.
“Across my last 40 robotic Ivor Lewis cases, I’ve had no anastomotic leaks.”
Costas Bizekis, MD
“Even when performed robotically, an Ivor Lewis esophagectomy isn’t a perfect solution,” Dr. Bizekis says. “But with experience, we’ve perfected our technique, especially for the anastomosis. Across my last 40 robotic Ivor Lewis cases, I’ve had no anastomotic leaks.”
Nationally Recognized Expertise
NYU Langone’s cardiothoracic surgery program has maintained a three-star rating for esophagectomy for esophageal cancer by the Society of Thoracic Surgeons for the past four years, which signifies the highest level of quality and above-average performance.
With no evidence of lymph node involvement or abdominopelvic metastasis, the patient will continue to be monitored with periodic CT scans for residual tumor growth.
The patient had only been home a few days when Dr. Bizekis received a text from his wife, saying: “He wants to go back to work. Is that okay?” Dr. Bizekis soon gave the patient the go-ahead. “Within just 10 days post-discharge, he was back at work and doing well, which is incredible,” Dr. Bizekis says.
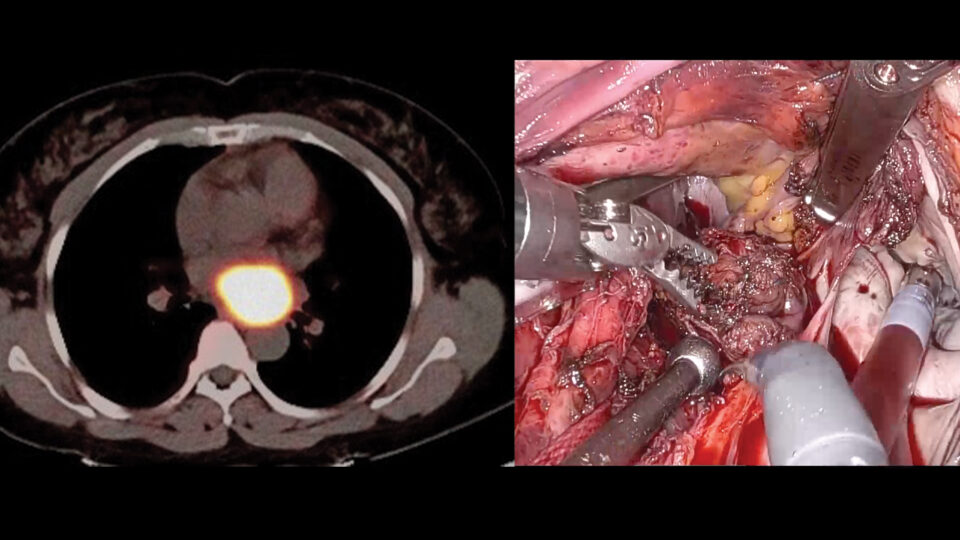
CT Imaging
CT showing distal esophageal wall thickening at the site of a known neoplasm. No evidence of abdominopelvic metastases. Source: NYU Langone Health
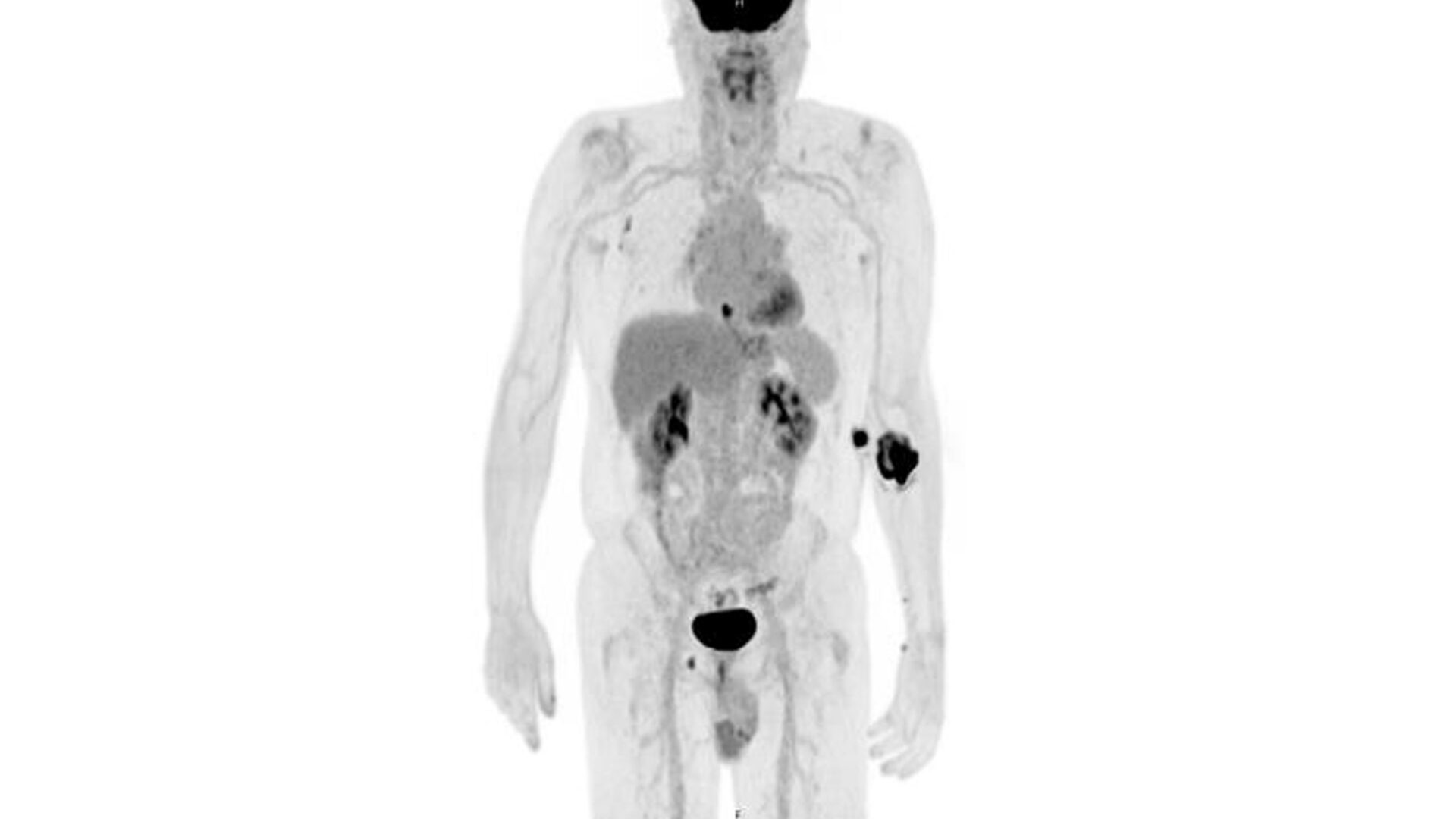
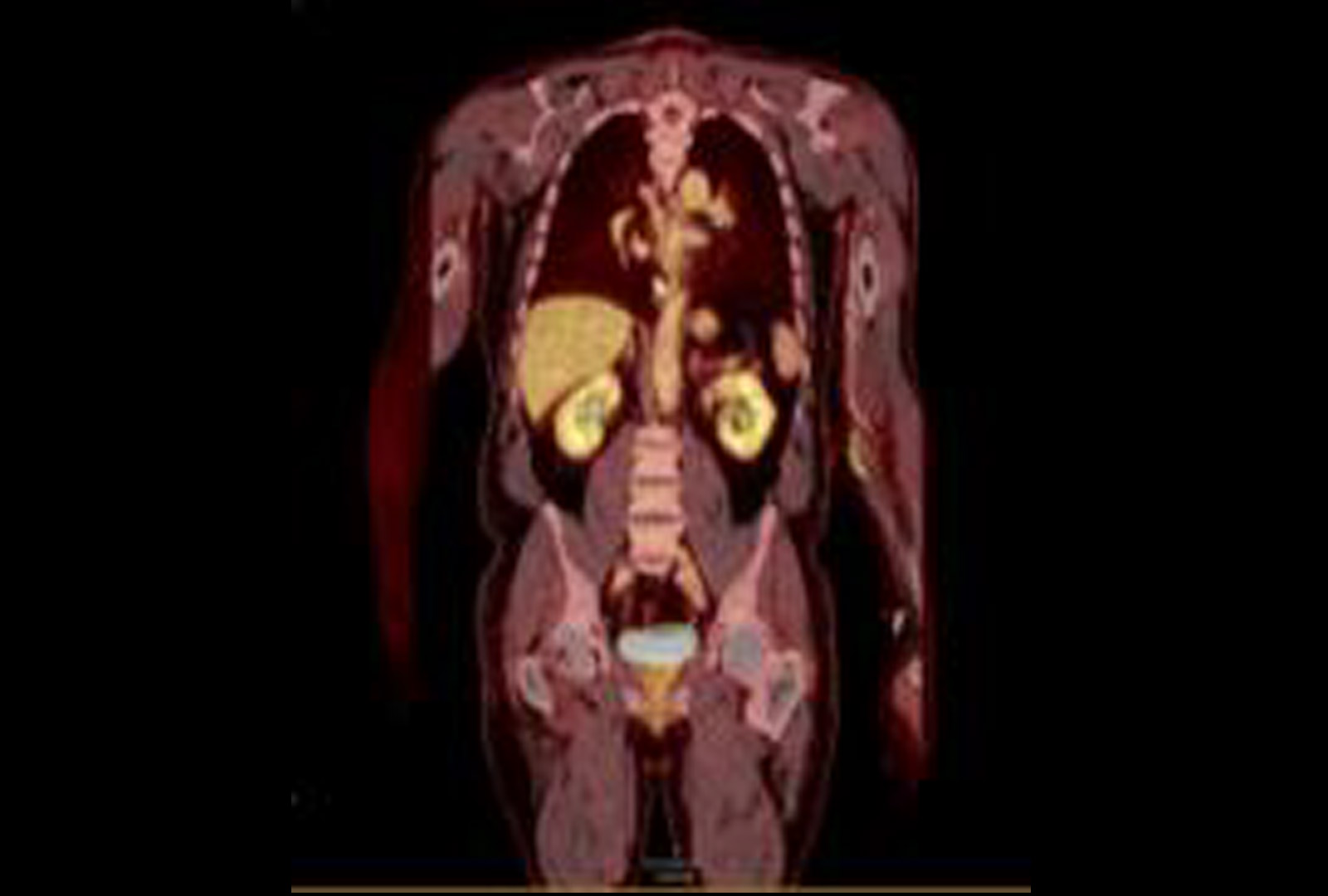
FDG Uptake
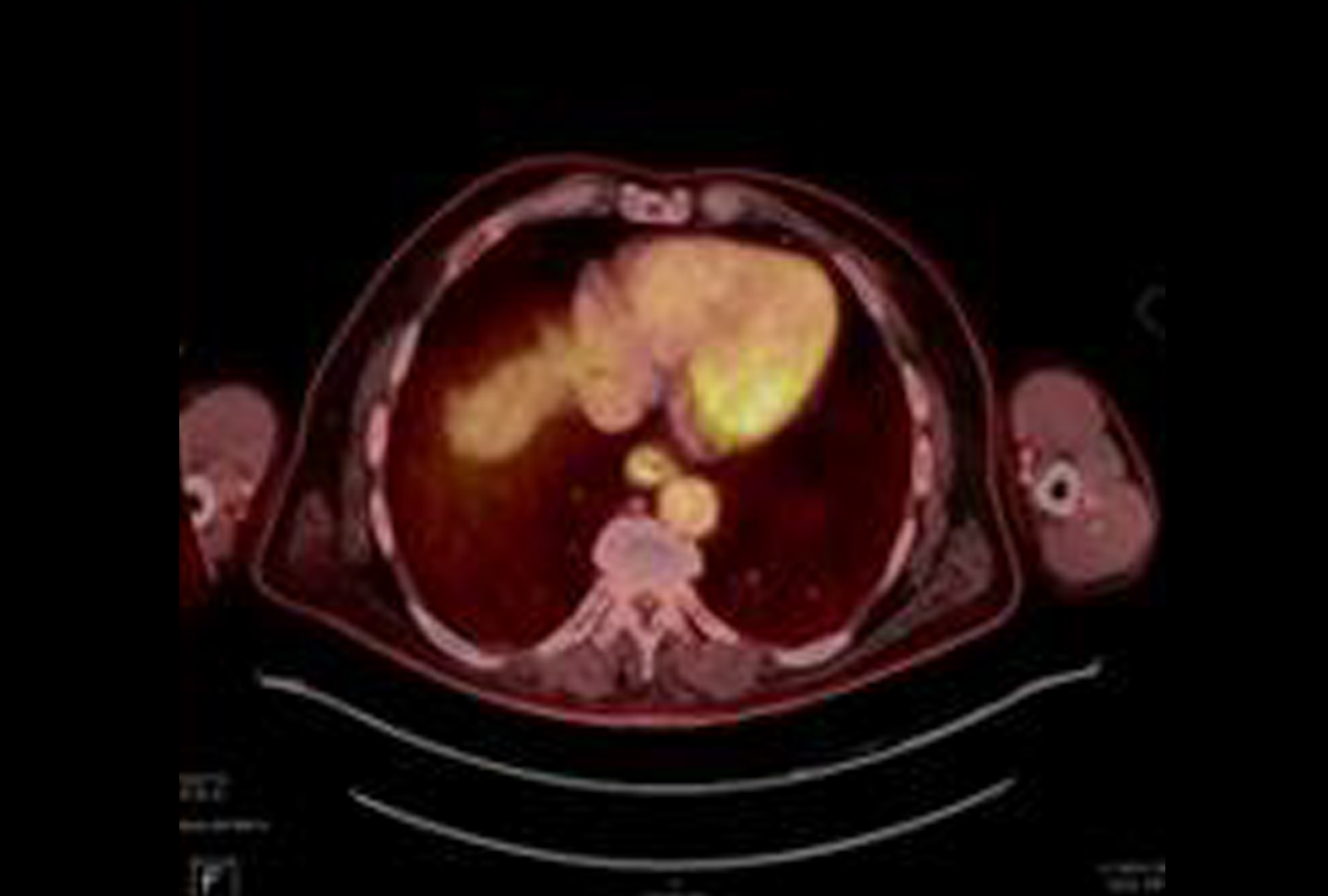
PET/CT showing FDG uptake at the distal esophagus, consistent with malignancy. There is also FDG uptake at the gastroesophageal junction, likely inflammatory or physiologic, along with FDG-avid bilateral hilar foci, right axillary nodes, and a right inguinal node—findings most consistent with inflammation. Source: NYU Langone Health
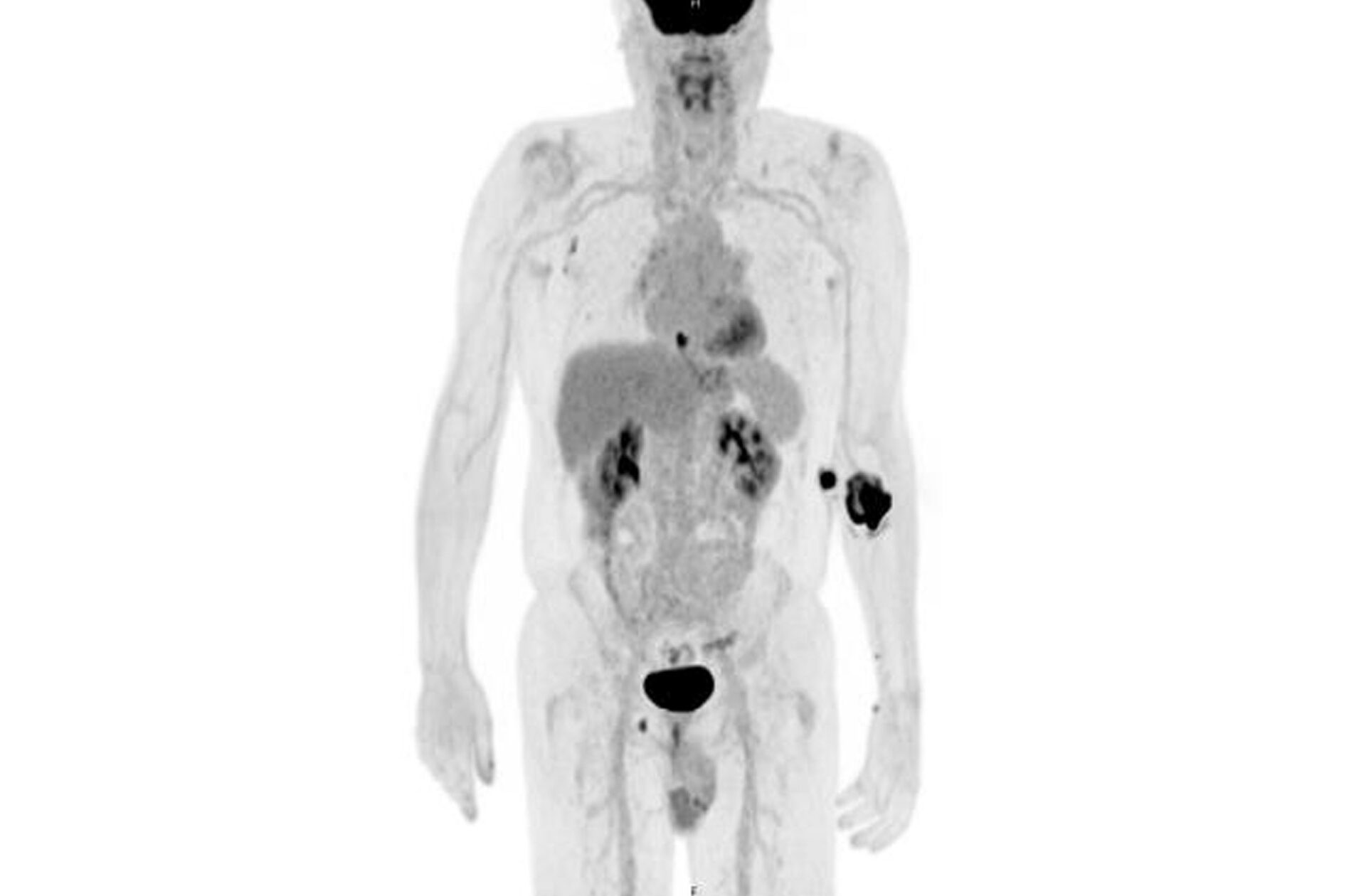
Further FDG Uptake in the Prostate
PET/CT demonstrating FDG uptake in the left basal to mid prostate correlating with elevated PSA. Source: NYU Langone Health